Review | Open Access | Volume 9 (Suppl 12): Article 05 | Published: 26 May 2026

Views: 1,044
Menu, Tables and Figures
| Year | Suspected Cases | Confirmed Cases | Positivity rate (%) | Probable Cases | Death (from Confirmed Cases) | Case Fatality Rate (%) | No. of Subnational levels affected |
|---|---|---|---|---|---|---|---|
| 2015 | 430 | 25 | 5.8 | – | 40 | *9.3 | 15 |
| 2016 | 921 | 109 | 11.8 | – | 119 | *12.9 | 29 |
| 2017 | 733 | 143 | 19.5 | – | 71 | *9.7 | 29 |
| 2018 | 3498 | 633 | 18.1 | 20 | 171 | 27.0 | 23 |
| 2019 | 5057 | 833 | 16.5 | 19 | 174 | 20.9 | 23 |
| 2020 | 6732 | 1181 | 17.5 | 14 | 244 | 20.7 | 27 |
| 2021 | 4654 | 510 | 11.0 | 6 | 102 | 20.0 | 17 |
| 2022 | 8202 | 1067 | 13.0 | 37 | 189 | 17.7 | 27 |
| 2023 | 9155 | 1270 | 13.9 | 12 | 227 | 17.9 | 28. |
| 2024 | 10098 | 1,309 | 13.0 | 23 | 214 | 16.3 | 28 |
| Total | 49,480 | 7,080 | 131 | 1,551 |
Table 1: Yearly Summary of Lassa Fever Cases from 2015 to 2024
| Demographics | 2015 | 2016 | 2017 | *2018 | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 |
|---|---|---|---|---|---|---|---|---|---|---|
| Age range (yrs) | – | – | – | – | <1 to 98 | <1 to 99 | <1 to70 | 1-90 | 1-93 | 1-98 |
| Predominant age (yrs) | – | – | – | 21–40 | 21–40 | 21–30 | 21–30 | 21-30 | 21-30 | 21-30 |
| Median age (yrs) | – | – | – | 32 | 34 | 30 | 29 | 30 | 32 | 32 |
| Male to female ratio | – | – | – | 1.6:1 | 1:1 | 1:0.9 | 1:0.9 | 1:0.8 | 1:0.9 | 1:1 |
Table 2: Demographic Characteristics of Lassa Fever Cases
| State | 2020 | 2021 | 2022 | 2023 | 2024 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % of total confirmed cases | Suspected | Confirmed | % of total confirmed cases | Suspected | Confirmed | % of total confirmed cases | |
| Abia | 62 | 5 | 0.4 | 11 | 1 | 0.2 | 23 | 0 | 0.0 | 17 | 0 | 0.0 | 20 | 0 | 0.0 |
| Adamawa | 21 | 4 | 0.3 | 8 | 0 | 0.0 | 19 | 1 | 0.1 | 19 | 1 | 0.1 | 21 | 3 | 0.2 |
| Akwa Ibom | 13 | 0 | 0.0 | 1 | 0 | 0.0 | 8 | 0 | 0.0 | 4 | 0 | 0.0 | 8 | 0 | 0.0 |
| Anambra | 35 | 2 | 0.1 | 10 | 1 | 0.2 | 41 | 5 | 0.5 | 42 | 3 | 0.2 | 47 | 4 | 0.3 |
| Bauchi | 410 | 52 | 4.4 | 164 | 39 | 7.6 | 1045 | 146 | 13.7 | 1048 | 194 | 15.3 | 1143 | 253 | 19.3 |
| Bayelsa | 7 | 0 | 0.0 | 3 | 0 | 0.0 | 8 | 0 | 0.0 | 41 | 2 | 0.2 | 27 | 2 | 0.2 |
| Benue | 108 | 10 | 0.8 | 34 | 8 | 1.6 | 289 | 39 | 3.7 | 198 | 40 | 3.1 | 1072 | 64 | 4.9 |
| Borno | 34 | 4 | 0.3 | 15 | 0 | 0.0 | 20 | 0 | 0.0 | 6 | 0 | 0.0 | 13 | 0 | 0.0 |
| Cross River | 14 | 0 | 0.0 | 4 | 1 | 0.2 | 20 | 4 | 0.4 | 29 | 2 | 0.2 | 64 | 8 | 0.6 |
| Delta | 166 | 18 | 1.5 | 50 | 1 | 0.2 | 84 | 4 | 0.4 | 64 | 4 | 0.3 | 100 | 5 | 0.4 |
| Ebonyi | 372 | 81 | 6.9 | 143 | 18 | 3.5 | 314 | 48 | 4.5 | 345 | 55 | 4.3 | 382 | 53 | 4.1 |
| Edo | 2765 | 380 | 32.2 | 2725 | 212 | 41.6 | 3210 | 273 | 25.6 | 3482 | 349 | 27.5 | 3103 | 289 | 22.1 |
| Ekiti | 20 | 0 | 0.0 | 3 | 0 | 0.0 | 4 | 1 | 0.1 | 20 | 0 | 0.0 | 17 | 0 | 0.0 |
| Enugu | 74 | 10 | 0.8 | 14 | 5 | 1.0 | 105 | 22 | 2.1 | 43 | 5 | 0.4 | 126 | 15 | 1.2 |
| FCT | 73 | 3 | 0.3 | 59 | 3 | 0.6 | 65 | 2 | 0.2 | 67 | 2 | 0.2 | 76 | 2 | 0.2 |
| Gombe | 56 | 9 | 0.8 | 22 | 0 | 0.0 | 251 | 24 | 2.2 | 86 | 10 | 0.8 | 64 | 5 | 0.4 |
| Imo | 22 | 0 | 0.0 | 9 | 1 | 0.2 | 56 | 1 | 0.1 | 19 | 1 | 0.1 | 41 | 3 | 0.2 |
| Jigawa | 30 | 0 | 0.0 | 12 | 0 | 0.0 | 9 | 0 | 0.0 | 25 | 3 | 0.2 | 26 | 2 | 0.2 |
| Kaduna | 132 | 7 | 0.6 | 53 | 8 | 1.6 | 94 | 4 | 0.4 | 43 | 1 | 0.1 | 127 | 15 | 1.2 |
| Kano | 26 | 5 | 0.4 | 24 | 0 | 0.0 | 41 | 1 | 0.1 | 63 | 6 | 0.5 | 58 | 1 | 0.08 |
| Katsina | 50 | 6 | 0.5 | 2 | 0 | 0.0 | 17 | 1 | 0.1 | 7 | 0 | 0.0 | 24 | 1 | 0.08 |
| Kebbi | 32 | 4 | 0.3 | 2 | 0 | 0.0 | 9 | 1 | 0.1 | 5 | 1 | 0.1 | 8 | 0 | 0.0 |
| Kogi | 117 | 40 | 3.4 | 17 | 3 | 0.6 | 142 | 49 | 4.6 | 48 | 11 | 0.9 | 158 | 37 | 2.8 |
| Kwara | 15 | 0 | 0.0 | 4 | 0 | 0.0 | 16 | 0 | 0.0 | 16 | 0 | 0.0 | 10 | 0 | 0.0 |
| Lagos | 33 | 1 | 0.1 | 16 | 0 | 0.0 | 52 | 1 | 0.1 | 29 | 2 | 0.2 | 49 | 1 | 0.08 |
| Nasarawa | 51 | 9 | 0.7 | 79 | 3 | 0.6 | 143 | 14 | 1.3 | 161 | 15 | 1.2 | 72 | 5 | 0.4 |
| Niger | 10 | 0 | 0.0 | 1 | 0 | 0.0 | 15 | 1 | 0.1 | 5 | 1 | 0.1 | 13 | 3 | 0.2 |
| Ogun | 40 | 1 | 0.1 | 3 | 0 | 0.0 | 20 | 0 | 0.0 | 26 | 0 | 0.0 | 39 | 1 | 0.08 |
| Ondo | 1494 | 423 | 35.8 | 1006 | 175 | 34.3 | 1683 | 348 | 32.6 | 2665 | 433 | 34.1 | 2613 | 400 | 30.6 |
| Osun | 36 | 2 | 0.2 | 3 | 0 | 0.0 | 8 | 0 | 0.0 | 8 | 0 | 0.0 | 8 | 0 | 0.0 |
| Oyo | 13 | 1 | 0.1 | 4 | 0 | 0.0 | 130 | 27 | 2.5 | 61 | 4 | 0.3 | 41 | 1 | 0.08 |
| Plateau | 181 | 32 | 2.7 | 42 | 9 | 1.8 | 102 | 11 | 1.0 | 113 | 20 | 1.6 | 115 | 17 | 1.3 |
| Rivers | 22 | 9 | 0.8 | 10 | 0 | 0.0 | 12 | 1 | 0.1 | 15 | 1 | 0.1 | 75 | 6 | 0.5 |
| Sokoto | 25 | 5 | 0.4 | 3 | 0 | 0.0 | 5 | 1 | 0.1 | 7 | 1 | 0.1 | 10 | 0 | 0.0 |
| Taraba | 150 | 58 | 4.9 | 72 | 22 | 4.3 | 106 | 37 | 3.5 | 314 | 102 | 8.0 | 301 | 112 | 8.6 |
| Yobe | 5 | 0 | 0.0 | 4 | 0 | 0.0 | 30 | 0 | 0.0 | 8 | 0 | 0.0 | 24 | 1 | 0.08 |
| Zamfara | 18 | 0 | 0.0 | 1 | 0 | 0.0 | 5 | 0 | 0.0 | 6 | 1 | 0.1 | 3 | 0 | 0.0 |
| Total | 6732 | 1181 | 100.0 | 4633 | 510 | 100.0 | 8201 | 1067 | 100.0 | 9155 | 1270 | 100.0 | 10,098 | 1309 | 100.0 |
Table 3: Distribution of Lassa Fever Results by States from 2020 – 2024<
| Region | 2020 | 2021 | 2022 | 2023 | 2024 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | |
| N/Central | 555 | 94 | 8.0 | 236 | 26 | 5.1 | 772 | 116 | 10.9 | 608 | 89 | 7.0 | 1,516 | 128 | 9.8 |
| N/East | 675 | 127 | 10.6 | 285 | 61 | 12.0 | 1471 | 208 | 19.5 | 1481 | 307 | 24.2 | 1,566 | 374 | 28.6 |
| N/West | 314 | 27 | 2.3 | 97 | 8 | 1.6 | 180 | 8 | 0.8 | 156 | 13 | 1.0 | 256 | 19 | 1.5 |
| S/East | 565 | 98 | 8.3 | 187 | 26 | 5.1 | 539 | 76 | 7.1 | 466 | 64 | 5.0 | 616 | 75 | 5.7 |
| S/South | 2987 | 407 | 34.5 | 2793 | 214 | 42.0 | 3342 | 282 | 26.4 | 3635 | 358 | 28.2 | 3,377 | 310 | 23.7 |
| S/West | 1636 | 428 | 36.2 | 1035 | 175 | 34.3 | 1897 | 377 | 35.3 | 2809 | 439 | 34.6 | 2,767 | 403 | 30.8 |
| Total | 6,732 | 1,181 | 100 | 4,633 | 510 | 100 | 8,201 | 1,067 | 100 | 9155 | 1,270 | 100 | 10,098 | 1,309 | 100 |
Table 4: Results of Lassa Fever by Geographical Zones
Zacchaeus Adeniran Adejuyigbe1,2,&, Item Inya Item1, Leviticus Dansura Mangpin1,2, Adama Abubakar Ahmad1, James Christopher Avong1, Muhammad Bashir Mika’il2, Jibril Imram2, Olajumoke Babatunde1, Adamu Ishaku Akyala2
1National Reference Laboratory, Nigeria Centre for Disease Control and Prevention, Abuja, Nigeria, 2Global Health and Infectious Disease Institute, Nasarawa State University, Keffi, Nasarawa State, Nigeria
&Corresponding author: Zacchaeus Adeniran Adejuyigbe, National Reference Laboratory, Nigeria Centre for Disease Control and Prevention, Abuja, Nigeria, Email: adezacks@gmail.com ORCID: https://orcid.org/0000-0003-2363-464X
Received: 26 Sep 2025, Accepted: 20 May 2026, Published: 21 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Lassa fever, case-definition, suspected case, confirmed case, case fatality rate
©Zacchaeus Adeniran Adejuyigbe et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Zacchaeus Adeniran Adejuyigbe et al., Epidemiological trend of Lassa fever in Nigeria, 2015-2024. Journal of Interventional Epidemiology and Public Health. 2026; 9(Suppl 12):5. https://doi.org/10.37432/jieph-d-25-00206
Introduction: Lassa fever remains a significant public health challenge in Nigeria, with a recent outbreak revealing the need for a new strategy to control and prevent the disease transmission. It is characterised by recurring outbreaks with high morbidity and mortality rates. It is endemic in several West African countries and is primarily transmitted through contact with Lassa virus on excreta of infected Mastomys rats. This review provided a comprehensive overview of the epidemiological trend, current situation and offers strategic recommendations for mitigating future outbreaks.
Methods: A retrospective analysis of epidemiological data on the burden of Lassa fever from 2015 to 2024 was conducted using data from the Nigeria Centre for Disease Control and Prevention (NCDC) website and other relevant sources to understand the epidemiological trend of the disease. Key variables analysed included demographic characteristics, geographical distribution, trends of the disease, and case fatality rates. The analysis was done using descriptive statistics.
Results: A total of 49,480 suspected Lassa fever cases were tested, of which 7,080 (14.3%) cases were laboratory confirmed in 29 states. Case fatality rates were between 9.3% and 27.0%. The predominant age group affected was 21-30 years, with a male: female ratio of 1.1:1. Median age was 31 years, and the range was between 0 and 98 years. Edo, Ondo, Taraba, Ebonyi, Bauchi, Plateau and Nasarawa states were most affected yearly. Lassa fever cases increased from 25 confirmed cases in 2015 to 1,309 in 2024. Yearly incidence of the disease peaked between weeks 1 and 13, with a sharp decline towards the middle of the year.
Conclusion: Lassa fever remains a significant public health concern in Nigeria, with rising incidence and high fatality rates. Targeted interventions are needed in hotspot states such as Edo, Ondo, and Taraba. Enhanced surveillance, early detection, and public health education should be categorized.
Lassa fever (LF) is an acute viral haemorrhagic illness first identified in 1969 in Lassa, Borno state, Nigeria. The disease is endemic in parts of West Africa, including Nigeria, where it has caused numerous outbreaks and resulting deaths. The Lassa virus is primarily transmitted to humans through contact with food or household items that have been contaminated by the urine or faeces of infected Mastomys rats. Human-to-human transmission can occur, particularly in healthcare settings lacking adequate infection control measures [1,2].
LF cases are categorized as suspected, confirmed and probable cases. According to the Nigeria Centre for Disease Control and Prevention – NCDC [3]. Suspected case refers to any individual presenting with one or more of the following: malaise, fever, headache, sore throat, cough, nausea, vomiting, diarrhoea, myalgia, chest pain, hearing loss and either (a) history of contact with excreta or urine of rodents (b) history of contact with a probable or confirmed Lassa fever case within a period of 2-21 days of onset of symptoms OR Any person with inexplicable bleeding/haemorrhagia. A confirmed case is defined as any suspected case supported by positive laboratory evidence such as the detection of viral RNA via polymerase chain reaction (PCR), or the presence of IgM antibody or viral isolation. Probable case is any suspected case who died or absconded without collection of specimens for laboratory testing. A contact is anyone who has been exposed to an infected person, or to an infected person’s secretions, excretions, or tissues within three weeks of last contact with a confirmed or probable case of Lassa fever.
The incubation period ranges from 2 to 21 days. Virus isolation through cell culture, PCR, immunofluorescence assay, complement fixation tests, enzyme‐linked immunosorbent assays for Lassa fever antigens and IgM antibodies, and lateral flow assays are different laboratory investigations that can be employed in the diagnosis, with reverse transcription PCR being the gold standard. Management of the disease is mainly supportive including fluid replacement for haemodynamic stability, dialysis in case of declining renal function and prophylactic antibiotics [4]. The specific antiviral therapy used till date is ribavirin. Ribavirin has been traditionally used for the treatment of Lassa fever. However, evidence supporting its use is insubstantial [5]. This review aims to explore a comprehensive overview of the epidemiological trend, current situation and offers strategic recommendations for mitigating future outbreaks.
A scoping retrospective epidemiological review of Lassa fever from 2015 to 2024 was carried out. Publicly available data from the Nigeria Centre for Disease Control and Prevention (NCDC) website and other relevant sources were utilized to present a comprehensive overview of the current situation and suggest strategies for mitigating future outbreaks. The epidemiological data from the NCDC website included Lassa fever yearly situation reports for weeks 1-52 of the years reviewed. Key variables analysed included demographic characteristics of cases, geographical distribution, seasonal trends, number of suspected/confirmed cases, and case fatality rates. The analysis was done using descriptive statistics.
Global epidemiology of Lassa fever
There have been imported cases of Lassa fever to the United States and Europe in travellers returning from endemic regions. These cases often resulted in isolated incidents rather than sustained outbreaks. The U.S. Centres for Disease Control and Prevention (CDC) reported several cases of Lassa fever in travellers returning from West Africa. One of the most notable cases was in 2015, when a case was confirmed in a U.S. traveller who had returned from Liberia [6]. In the United Kingdom, three cases of Lassa fever were reported in 2022 in travellers who had returned from West Africa, of which one of the patients sadly died [7].
Historically, there have also been cases of Lassa fever in Germany and the Netherlands involving individuals who had been to endemic areas in West Africa [7]. In 2016, there were three cases of Lassa fever reported in EU/EEA countries – Germany reported two cases, and Sweden reported one case [8]. Germany recorded a fatal case of Lassa fever in 2016 in a person who had been evacuated to Cologne, Germany, from Togo. These cases revealed the risks of Lassa fever spreading to non-endemic regions through travellers. [8,9,10]. The Netherlands has also reported occasional cases of Lassa fever imported by travellers. However, these were typically isolated incidents with no further transmission [11].
Lassa fever in Africa
The disease primarily affects West Africa, especially Nigeria, Benin, Ghana, Guinea, Liberia, Mali, and Sierra Leone [12]. It is mainly transmitted through contact with the urine or faeces of infected Mastomys natalensis rodents, while human-to-human transmission can occur in healthcare settings without adequate infection control measures [13|. Nigeria experiences the highest number of cases annually, particularly during the dry season (November to April) [3]. Lassa fever causes an estimated 100,000 to 300,000 cases and approximately 5,000 deaths per year, though the true burden may be higher due to underreporting and limited diagnostic capabilities [14].
Lassa fever disproportionately affects pregnant women, especially in the third trimester, where foetal death and maternal death rates can exceed 80% and 30%, respectively [15]. Nosocomial transmission is also a concern, hence the need for stringent infection prevention and control (IPC) measures [16].
The antiviral ribavirin is the primary treatment but is most effective when administered early [17]. Although vaccine development is ongoing, no licensed vaccine is currently available [18]. Key control strategies include improving rodent control, enhancing diagnostic capacity and surveillance efforts [19]
Situational analysis of Lassa fever in Nigeria
Table 1 shows the yearly summary of Lassa fever cases from 2015 to 2024, which includes the number of suspected cases, confirmed cases, probable cases, case fatality rates and the number of states affected. A total of 49,480 cases were suspected to be infected with Lassa fever, out of which 7,080 cases were laboratory-confirmed to have the disease in at most 29 states. The overall proportion of confirmed cases was 14.3%. The number of confirmed cases increased over time from 25 in 2015 to 1,309 cases in 2024. This could be due to enhanced surveillance, active contact tracing, as well as more laboratory testing put in place in the country. The proportion of confirmed cases in the number of suspected cases was highest (19.5%) in 2017, and this was followed by 18.1% in the year 2018.
The lowest case fatality rate (CFR) (9.3%) was recorded in 2015, while 2018 recorded the highest CFR of 27.0%. Meanwhile, there have been varying case fatality rates in the years under review. The number of states affected since 2015 was at least 15 states, with the highest being 29 states affected in 2016. Meanwhile, the outbreak of the disease in 2023 and 2024 was in 28 states, representing the recent number of affected states. Edo and Ondo states bear the highest burden from 2018 through to 2024. An analysis of the burden of Lassa fever in Edo and Ondo states combined revealed that from year 2018 to 2024, both states accounted for 69% (2018), 68% (2019), 68% (2020), 76% (2021), 58% (2022), 61% (2023), and 53% (2024) of the total confirmed cases of Lassa fever of all the states affected. Other states included Ebonyi, Bauchi, Taraba, and Plateau, amongst other states.
Overall, the ages of affected cases as shown in Table 2 ranged from 0 to 98 years. The predominant ages were from 21 to 30 years, and the median age ranged from 29 to 34 years. The affected number of males as compared to their female countered were relative. Although there were differences in the ratio of male to female in 2018 (1.6:1), 2022 (1:0.8), 2020, 2021 and 2023 had 1:0.9 as the male: female ratio.
Table 3 shows the distribution of the confirmed cases of LF from 2020 to 2024, though there were no sufficient data from sources reviewed to account for the distribution of confirmed cases of the disease in each state from 2015 to 2019 by state; only cumulative data for these years were available. The confirmed cases of Lassa fever have been steadily high for Edo and Ondo states. Others include Bauchi, Ebonyi, Taraba and Plateau state. The number of suspected cases was very low in 2021; this may be as a result of the COVID-19 pandemic, which shifted most of the attention from Lassa fever to SARS-CoV-2 surveillance and testing.
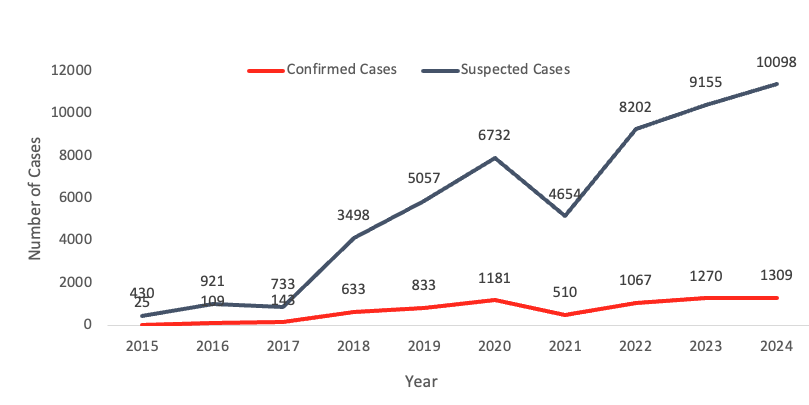
The South-south and South-west recorded the highest proportion of total confirmed cases (Table 4). This is not disconnected from the high number of confirmed cases recorded in Edo and Ondo states, which are from the south-south and south-western regions, respectively. Other regions include north-east, north central and south-east. The least proportion of total confirmed cases was recorded in the North-west in 2020 through 2024. The trend of suspected and confirmed cases from 2015 to 2024 showed that the cases of the disease increased over time (Figure 1).
Contributing factors to the burden of Lassa fever
Poor environmental and socioeconomic conditions
Poor sanitation, inadequate waste management, and crowded living conditions in many parts of Nigeria create an ideal environment for the proliferation of Mastomys rats. These conditions increase the likelihood of rodent-human interactions, thereby heightening the risk of transmission [3]. Additionally, poverty and food insecurity lead to behaviours such as consuming bush meat and inadequate food storage, which further expose people to the virus [21].
Inadequate healthcare infrastructure
Nigeria’s healthcare system faces significant challenges, including inadequate infection control practices, limited resources, and insufficient training for healthcare workers. These deficiencies are particularly problematic during outbreaks, leading to higher transmission rates and fatalities, especially among healthcare personnel [3]. The lack of personal protective equipment (PPE) and poor hospital hygiene standards exacerbate the spread of the virus within healthcare settings [22].
Challenges impeding surveillance and response
Despite improvements in disease surveillance and response mechanisms, significant gaps remain. Effective disease monitoring and rapid response are critical to controlling outbreaks, yet issues such as insufficient funding, logistical challenges, and inadequate coordination persist [3]. The limited capacity for laboratory diagnosis across the country and factors affecting prompt testing of suspected cases negatively affect timely treatment and control measures [23]. Despite some efforts to control the disease, Mastomys rat is highly abundant and well adapted to the environment, especially in rural areas where seasonal migration of the rat is a critical factor [28]. Open refuse dumps, as well as traditional food drying on the ground in open spaces, facilitate human-rodent interaction. This has posed a serious challenge in the control of the disease over the years.
Detection and diagnostic methods
Clinical diagnosis
Clinical diagnosis of Lassa fever is challenging due to its nonspecific symptoms, which overlap with other febrile illnesses such as malaria and typhoid fever. Symptoms typically include fever, general weakness, headache, sore throat, muscle pain, chest pain, nausea, vomiting, diarrhea, and abdominal pain [24]. Severe cases can present with haemorrhagic symptoms and multi-organ dysfunction.
Laboratory diagnosis
Accurate diagnosis of Lassa fever requires laboratory confirmation. The following are the main methods used:
RT-PCR is the gold standard for the early detection of Lassa virus RNA in blood samples. It is highly sensitive and specific, allowing for the identification of the virus within the first few days of symptom onset. RT-PCR can also be used to monitor viral load and response to treatment [25].
ELISA is used to detect Lassa virus-specific antibodies (IgM and IgG) in patient serum. IgM antibodies are detectable early in the course of infection, while IgG antibodies indicate a past infection or longer duration of illness. ELISA can also detect Lassa virus antigens, providing another means of confirming infection [24].
Virus isolation involves culturing the Lassa virus from patient samples in specialized laboratory facilities. This method is highly specific but requires advanced biosafety containment [(Biosafety Level 4 (BSL-4) laboratory] and is not routinely used due to the high risk of laboratory-acquired infections [1].
Public health response and key recommendations
Enhanced surveillance
The NCDC, as the national public health institute, has improved reporting systems and data collection methods for the monitoring and tracking of the spread of Lassa fever more effectively. The integration of real-time data collection tools (such as Surveillance Outbreak Response Management and Analysis System – SORMAS) and geographic information systems (GIS) has enabled more precise mapping of outbreaks and resource allocation [26]. Enhanced surveillance efforts have led to better identification and management of cases [3].
Prompt testing and reporting:
There is a critical need to improve prompt testing through the inclusion of rapid diagnostic tests (RDT) that show significant sensitivity and specificity [29], while maintaining a high standard of biosafety measures. This, however, can not replace the use of polymerase chain reaction – PCR, which remains the gold-standard. A tiered diagnostic framework integrating RDT screening with qRT-PCR confirmation will enhance prompt detection, accuracy, accelerated outbreak response, and will strengthen surveillance. Therefore, a testing strategy that follows a well mapped-out testing algorithm/flow should be developed where all RDT-negative tests can be done via PCR, and results are promptly reported via the real-time reporting system developed by the NCDC.
Community engagement
Public health campaigns aimed at raising awareness about Lassa fever, its transmission, and preventive measures have been crucial. Community engagement efforts include educating the public on proper food storage practices and the importance of rodent control. Initiatives such as distributing rodent-proof containers and promoting safe handling of food and water are vital in reducing exposure [3]. There is a need to educate the public on the need to dispose waste properly – which is a major attraction point for Mastomys rats. Communities should be enlightened on the peak season for the proliferation of Mastomys rats, which occurs at the start of dry season, and how to put measures in place against the disease. [28].
Local support from the government:
There is a need for more support from the local, state, and federal governments in the campaign against the deadly disease. These supports can be achieved through positive and sustained political will, direct sponsorships of programs aimed at educating community residents, creating environment that discourages the proliferation of Mastomys rats (for example, enforcing strict laws that discourage indiscriminate disposal of wastes), expansion of testing sites/laboratories, provision of grants for translational research, and other financial support for prompt outbreak response.
Healthcare worker training
Training programs for healthcare workers focus on infection control and patient management to reduce the risk of transmission within healthcare settings. These programs are essential in protecting healthcare workers and ensuring the safe treatment of patients [3]. Workshops and simulation exercises on the use of personal protective equipment (PPE), isolation protocols, and the management of Lassa fever cases are part of these training efforts [26].
Research and development
Ongoing research is vital to understanding Lassa fever better. Prevention strategies, developing effective treatments and vaccines are important approaches in tackling the disease. Collaborative efforts between local and international stakeholders and research institutions can advance knowledge and improve public health responses [27]. Research that focuses on understanding the virus’s genetic diversity across different geographical locations, transmission dynamics, development of cost-effective genomic testing approaches that embrace shorter turn-around time, and potential therapeutic targets should be employed [4].
Lassa fever has continued to remain a significant public health challenge in Nigeria with a high mortality rate. The disease continues to pose immense health security challenges to other West African countries and beyond. There has been a continuous yearly increase in Lassa fever cases despite interventions and measures put in place to mitigate the menace of the disease. South-southern and South-western states require urgent, critical measures to address the ever-increasing number of cases of the disease, as the two geographical regions record a yearly high number of cases. Addressing underlying environmental conditions, strengthening healthcare responses, and engaging communities are critical steps toward mitigating the impact of the disease.
What is already known about the topic
What this study adds
ZAA: Conceptualisation, data curation, formal analysis, methodology, resources, supervision, validation, writing-original draft, writing -review & editing
LDM: writing -review & editing
AAA: writing -review & editing
III: writing -review & editing
JCA: Visualisation, writing -review & editing
AIA: writing -review & editing, Supervision
JI: writing -review & editing
MBM: writing -review & editing
| Year | Suspected Cases | Confirmed Cases | Positivity rate (%) | Probable Cases | Death (from Confirmed Cases) | Case Fatality Rate (%) | No. of Subnational levels affected |
|---|---|---|---|---|---|---|---|
| 2015 | 430 | 25 | 5.8 | – | 40 | *9.3 | 15 |
| 2016 | 921 | 109 | 11.8 | – | 119 | *12.9 | 29 |
| 2017 | 733 | 143 | 19.5 | – | 71 | *9.7 | 29 |
| 2018 | 3498 | 633 | 18.1 | 20 | 171 | 27.0 | 23 |
| 2019 | 5057 | 833 | 16.5 | 19 | 174 | 20.9 | 23 |
| 2020 | 6732 | 1181 | 17.5 | 14 | 244 | 20.7 | 27 |
| 2021 | 4654 | 510 | 11.0 | 6 | 102 | 20.0 | 17 |
| 2022 | 8202 | 1067 | 13.0 | 37 | 189 | 17.7 | 27 |
| 2023 | 9155 | 1270 | 13.9 | 12 | 227 | 17.9 | 28. |
| 2024 | 10098 | 1,309 | 13.0 | 23 | 214 | 16.3 | 28 |
| Total | 49,480 | 7,080 | 131 | 1,551 |
| Demographics | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 |
|---|---|---|---|---|---|---|---|---|---|---|
| Age range (yrs) | – | – | – | – | <1 to 98 | <1 to 99 | <1 to70 | 1-90 | 1-93 | 1-98 |
| Predominant age (yrs) | – | – | – | 21–40 | 21–40 | 21–30 | 21–30 | 21-30 | 21-30 | 21-30 |
| Median age (yrs) | – | – | – | 32 | 34 | 30 | 29 | 30 | 32 | 32 |
| Male to female ratio | – | – | – | 1.6:1 | 1:1 | 1:0.9 | 1:0.9 | 1:0.8 | 1:0.9 | 1:1 |
| State | 2020 | 2021 | 2022 | 2023 | 2024 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % of total confirmed cases | Suspected | Confirmed | % of total confirmed cases | Suspected | Confirmed | % of total confirmed cases | |
| Abia | 62 | 5 | 0.4 | 11 | 1 | 0.2 | 23 | 0 | 0.0 | 17 | 0 | 0.0 | 20 | 0 | 0.0 |
| Adamawa | 21 | 4 | 0.3 | 8 | 0 | 0.0 | 19 | 1 | 0.1 | 19 | 1 | 0.1 | 21 | 3 | 0.2 |
| Akwa Ibom | 13 | 0 | 0.0 | 1 | 0 | 0.0 | 8 | 0 | 0.0 | 4 | 0 | 0.0 | 8 | 0 | 0.0 |
| Anambra | 35 | 2 | 0.1 | 10 | 1 | 0.2 | 41 | 5 | 0.5 | 42 | 3 | 0.2 | 47 | 4 | 0.3 |
| Bauchi | 410 | 52 | 4.4 | 164 | 39 | 7.6 | 1045 | 146 | 13.7 | 1048 | 194 | 15.3 | 1143 | 253 | 19.3 |
| Bayelsa | 7 | 0 | 0.0 | 3 | 0 | 0.0 | 8 | 0 | 0.0 | 41 | 2 | 0.2 | 27 | 2 | 0.2 |
| Benue | 108 | 10 | 0.8 | 34 | 8 | 1.6 | 289 | 39 | 3.7 | 198 | 40 | 3.1 | 1072 | 64 | 4.9 |
| Borno | 34 | 4 | 0.3 | 15 | 0 | 0.0 | 20 | 0 | 0.0 | 6 | 0 | 0.0 | 13 | 0 | 0.0 |
| Cross River | 14 | 0 | 0.0 | 4 | 1 | 0.2 | 20 | 4 | 0.4 | 29 | 2 | 0.2 | 64 | 8 | 0.6 |
| Delta | 166 | 18 | 1.5 | 50 | 1 | 0.2 | 84 | 4 | 0.4 | 64 | 4 | 0.3 | 100 | 5 | 0.4 |
| Ebonyi | 372 | 81 | 6.9 | 143 | 18 | 3.5 | 314 | 48 | 4.5 | 345 | 55 | 4.3 | 382 | 53 | 4.1 |
| Edo | 2765 | 380 | 32.2 | 2725 | 212 | 41.6 | 3210 | 273 | 25.6 | 3482 | 349 | 27.5 | 3103 | 289 | 22.1 |
| Ekiti | 20 | 0 | 0.0 | 3 | 0 | 0.0 | 4 | 1 | 0.1 | 20 | 0 | 0.0 | 17 | 0 | 0.0 |
| Enugu | 74 | 10 | 0.8 | 14 | 5 | 1.0 | 105 | 22 | 2.1 | 43 | 5 | 0.4 | 126 | 15 | 1.2 |
| FCT | 73 | 3 | 0.3 | 59 | 3 | 0.6 | 65 | 2 | 0.2 | 67 | 2 | 0.2 | 76 | 2 | 0.2 |
| Gombe | 56 | 9 | 0.8 | 22 | 0 | 0.0 | 251 | 24 | 2.2 | 86 | 10 | 0.8 | 64 | 5 | 0.4 |
| Imo | 22 | 0 | 0.0 | 9 | 1 | 0.2 | 56 | 1 | 0.1 | 19 | 1 | 0.1 | 41 | 3 | 0.2 |
| Jigawa | 30 | 0 | 0.0 | 12 | 0 | 0.0 | 9 | 0 | 0.0 | 25 | 3 | 0.2 | 26 | 2 | 0.2 |
| Kaduna | 132 | 7 | 0.6 | 53 | 8 | 1.6 | 94 | 4 | 0.4 | 43 | 1 | 0.1 | 127 | 15 | 1.2 |
| Kano | 26 | 5 | 0.4 | 24 | 0 | 0.0 | 41 | 1 | 0.1 | 63 | 6 | 0.5 | 58 | 1 | 0.08 |
| Katsina | 50 | 6 | 0.5 | 2 | 0 | 0.0 | 17 | 1 | 0.1 | 7 | 0 | 0.0 | 24 | 1 | 0.08 |
| Kebbi | 32 | 4 | 0.3 | 2 | 0 | 0.0 | 9 | 1 | 0.1 | 5 | 1 | 0.1 | 8 | 0 | 0.0 |
| Kogi | 117 | 40 | 3.4 | 17 | 3 | 0.6 | 142 | 49 | 4.6 | 48 | 11 | 0.9 | 158 | 37 | 2.8 |
| Kwara | 15 | 0 | 0.0 | 4 | 0 | 0.0 | 16 | 0 | 0.0 | 16 | 0 | 0.0 | 10 | 0 | 0.0 |
| Lagos | 33 | 1 | 0.1 | 16 | 0 | 0.0 | 52 | 1 | 0.1 | 29 | 2 | 0.2 | 49 | 1 | 0.08 |
| Nasarawa | 51 | 9 | 0.7 | 79 | 3 | 0.6 | 143 | 14 | 1.3 | 161 | 15 | 1.2 | 72 | 5 | 0.4 |
| Niger | 10 | 0 | 0.0 | 1 | 0 | 0.0 | 15 | 1 | 0.1 | 5 | 1 | 0.1 | 13 | 3 | 0.2 |
| Ogun | 40 | 1 | 0.1 | 3 | 0 | 0.0 | 20 | 0 | 0.0 | 26 | 0 | 0.0 | 39 | 1 | 0.08 |
| Ondo | 1494 | 423 | 35.8 | 1006 | 175 | 34.3 | 1683 | 348 | 32.6 | 2665 | 433 | 34.1 | 2613 | 400 | 30.6 |
| Osun | 36 | 2 | 0.2 | 3 | 0 | 0.0 | 8 | 0 | 0.0 | 8 | 0 | 0.0 | 8 | 0 | 0.0 |
| Oyo | 13 | 1 | 0.1 | 4 | 0 | 0.0 | 130 | 27 | 2.5 | 61 | 4 | 0.3 | 41 | 1 | 0.08 |
| Plateau | 181 | 32 | 2.7 | 42 | 9 | 1.8 | 102 | 11 | 1.0 | 113 | 20 | 1.6 | 115 | 17 | 1.3 |
| Rivers | 22 | 9 | 0.8 | 10 | 0 | 0.0 | 12 | 1 | 0.1 | 15 | 1 | 0.1 | 75 | 6 | 0.5 |
| Sokoto | 25 | 5 | 0.4 | 3 | 0 | 0.0 | 5 | 1 | 0.1 | 7 | 1 | 0.1 | 10 | 0 | 0.0 |
| Taraba | 150 | 58 | 4.9 | 72 | 22 | 4.3 | 106 | 37 | 3.5 | 314 | 102 | 8.0 | 301 | 112 | 8.6 |
| Yobe | 5 | 0 | 0.0 | 4 | 0 | 0.0 | 30 | 0 | 0.0 | 8 | 0 | 0.0 | 24 | 1 | 0.08 |
| Zamfara | 18 | 0 | 0.0 | 1 | 0 | 0.0 | 5 | 0 | 0.0 | 6 | 1 | 0.1 | 3 | 0 | 0.0 |
| Total | 6732 | 1181 | 100.0 | 4633 | 510 | 100.0 | 8201 | 1067 | 100.0 | 9155 | 1270 | 100.0 | 10,098 | 1309 | 100.0 |
| Region | 2020 | 2021 | 2022 | 2023 | 2024 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | Suspected | Confirmed | % Pos of total confirmed cases | |
| N/Central | 555 | 94 | 8.0 | 236 | 26 | 5.1 | 772 | 116 | 10.9 | 608 | 89 | 7.0 | 1,516 | 128 | 9.8 |
| N/East | 675 | 127 | 10.6 | 285 | 61 | 12.0 | 1471 | 208 | 19.5 | 1481 | 307 | 24.2 | 1,566 | 374 | 28.6 |
| N/West | 314 | 27 | 2.3 | 97 | 8 | 1.6 | 180 | 8 | 0.8 | 156 | 13 | 1.0 | 256 | 19 | 1.5 |
| S/East | 565 | 98 | 8.3 | 187 | 26 | 5.1 | 539 | 76 | 7.1 | 466 | 64 | 5.0 | 616 | 75 | 5.7 |
| S/South | 2987 | 407 | 34.5 | 2793 | 214 | 42.0 | 3342 | 282 | 26.4 | 3635 | 358 | 28.2 | 3,377 | 310 | 23.7 |
| S/West | 1636 | 428 | 36.2 | 1035 | 175 | 34.3 | 1897 | 377 | 35.3 | 2809 | 439 | 34.6 | 2,767 | 403 | 30.8 |
| Total | 6,732 | 1,181 | 100 | 4,633 | 510 | 100 | 8,201 | 1,067 | 100 | 9155 | 1,270 | 100 | 10,098 | 1,309 | 100 |