Research | Open Access | Volume 9 (2): Article 86 | Published: 29 May 2026

Views: 599
Menu, Tables and Figures
| Indicator | Numerator | Denominator | Target |
|---|---|---|---|
| Non-polio AFP rate | # Cases discarded as NPFPR in children aged <15 | # Population aged <15 years | ≥2 |
| Stool adequacy | # of 2 stool specimens collected ≥24 hours apart, within ≤14 days of onset of paralysis | # AFP cases | ≥80% |
| Stool Condition | # AFP cases with two stools that arrived in good condition at the WHO-accredited lab | # AFP cases | ≥80% |
| Non-Polio Enterovirus | # of AFP cases with enterovirus | # AFP cases | ≥10% |
| Timeliness of Investigation | # AFP cases with ≤48 hours between notification and investigation | # AFP cases | ≥80% |
| Timeliness of stool specimen shipment | # AFP cases with ≤3 days between stool collection and arrival at the WHO-accredited lab | # AFP cases | ≥80% |
Table 1: AFP surveillance Key Performance Indicators
| Characteristics | Frequency (%) |
|---|---|
| Sex | |
| Male | 8 (38.1) |
| Female | 13 (61.9) |
| Age | |
| 20-30 | 12 (57.1) |
| 31-40 | 8 (38.1) |
| Above 40 | 1 (4.8) |
| Designation | |
| Disease Control Officer | 6 (28.5) |
| Nurse | 11 (52.4) |
| Physician Assistant | 1 (4.8) |
| Field assistant | 2 (9.5) |
| Public Health Nurse | 1 (4.8) |
Table 2: Demographic characteristics of study participants
| Name of Case-Based Form | # Of variables | # Of variable properly filled | # Of missing variable | # Of improperly filled variable | Completeness (%) |
|---|---|---|---|---|---|
| GHA-VOL-HOV-017-001 | 44 | 32 | 12 | 0 | 72.7 |
| GHA-VOL-HOV-017-002 | 44 | 32 | 12 | 0 | 72.7 |
| GHA-VOL-HOV-018-001 | 44 | 32 | 12 | 0 | 72.7 |
| GHA-VOL-HOV-019-001 | 75 | 50 | 25 | 0 | 66.6 |
| GHA-VOL-HOV-2020-001 | 75 | 50 | 25 | 0 | 66.6 |
| GHA-VOL-HOV-2020-002 | 75 | 50 | 25 | 0 | 66.6 |
| GHA-VOL-HOV-2021-001 | 75 | 50 | 25 | 0 | 66.6 |
| GHA-VOL-HOV-2021-002 | 75 | 49 | 26 | 0 | 65.3 |
| GHA-VOL-HOV-2021-003 | 75 | 49 | 26 | 0 | 65.3 |
| GHA-VOL-HOV-2021-004 | 75 | 49 | 26 | 0 | 65.3 |
| Overall | 68.04 | ||||
Table 3: Completeness of the Case-Based Form, Ho Municipality, 2017-2021
| Case-Based Form | Specimens collected 24-48 hrs apart | Specimen sent to the Ref lab |
|---|---|---|
| GHA-VOL-HOV-017-001 | T | L |
| GHA-VOL-HOV-017-002 | T | L |
| GHA-VOL-HOV-018-001 | T | L |
| GHA-VOL-HOV-019-001 | T | L |
| GHA-VOL-HOV-2020-001 | T | L |
| GHA-VOL-HOV-2020-002 | T | L |
| GHA-VOL-HOV-2021-001 | T | NR |
| GHA-VOL-HOV-2021-002 | T | NR |
| GHA-VOL-HOV-2021-003 | T | NR |
| GHA-VOL-HOV-2021-004 | T | T |
| Overall Timeliness (%) | 100% | 10% |
T= Timely, L = Late, NR= Not recorded
Table 4: Timeliness of AFP surveillance, Ho Municipality, 2017-2021
| Variable | Value, n (%) |
|---|---|
| Sex | |
| Male | 4 (40) |
| Female | 6 (60) |
| Age (years) | |
| <5 | 7 (70) |
| 5-10 | 2 (20) |
| >10 | 1 (10) |
| Vaccination status (OPV doses) | |
| 1-3 | 4 (40) |
| ≥4 | 4 (40) |
| Unknown | 2 (20) |
| Clinical characteristics | |
| Fever | 3 (23.1) |
| Asymmetric paralysis | 1 (7.7) |
| Rapid progression of paralysis | 9 (69.2) |
Table 5: Representativeness of AFP Cases, Ho Municipality, January 2017–December 2021
Bakalilu Kijera1,&, Abdul Nasir Alhasan2, Sarja Jarjusey1, Mary Bobb1, Lamin Manjang1, Donne Ameme1, Charles Lwanga Noora1, Delia Bandoh1, Ernest Kenu1
1Ghana Field Epidemiology and Laboratory Training Programme, School of Public Health, University of Ghana, Legon, Ghana, 2Ghana Health Services, Accra, Ghana
&Corresponding author: Bakalilu Kijera, Ghana Field Epidemiology and Laboratory Training Programme, School of Public Health, University of Ghana, Legon, Ghana, Email: bkkijera@gmail.com ORCID: https://orcid.org/0009-0006-0055-147X
Received: 17 Apr 2025, Accepted: 26 May 2026, Published: 29 May 2026
Domain: Infectious Disease Epidemiology
Keywords: Acute Flaccid Paralysis, surveillance system evaluation, Ho Municipality, Ghana
©Bakalilu Kijera et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Bakalilu Kijera et al., Acute flaccid paralysis surveillance system evaluation, Ho Municipality, Volta Region, Ghana. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):86. https://doi.org/10.37432/jieph-d-25-00093
Introduction: Ghana reported the last indigenous case of wild poliovirus causing poliomyelitis in 1999. However, Ghana experienced another outbreak when cases were imported into the country in 2003 and 2004. Ghana’s decade-long polio-free status ended in 2019 with the detection of circulating vaccine-derived polio virus type 2 (cVDPV2) through environmental surveillance. This evaluation describes the usefulness and attributes of an acute flaccid paralysis (AFP) surveillance system and whether the system meets its objectives.
Methods: A descriptive evaluation of the AFP surveillance system from January 2017 to December 2021 was conducted in Ho Municipality, Volta Region. Interviews with health workers and key stakeholders, observations, review of records, and administration of semi-structured questionnaires were conducted. The Centres for Disease Control and Prevention updated guidelines for evaluating public health surveillance systems were used as a reference for developing a checklist. The quantitative data were analysed using summary statistics and presented in percentages and frequencies. The qualitative interviews were audio recorded, transcribed, and narratively analysed.
Results: Ten AFP cases were reported from January 2017 to December 2021. The average Non-Polio Acute Flaccid Paralysis (NP-AFP) rate was 2.14 per 100,000, with a minimum of 1.09 and a maximum of 4.12 per 100,000 population under 15 years. One (10.0%) of the specimens reached the reference lab within 72 hours, and an overall completeness of 68.0%. The non-polio enterovirus (NPENT) detection rate was 0% from 2018 to 2021. Overall, only 20% (2/10) had NPENT in the stool.
Conclusion: The AFP surveillance system in Ho municipality is partially meeting its objectives. It demonstrates partial sensitivity but is poor in timeliness and completeness. The District Health Management Team should ensure specimens are sent to the reference laboratory within 72 hours after the case investigation.
Poliomyelitis is a contagious disease caused by the poliovirus that often affects children under 15 years of age [1] . Poliovirus can spread from person to person through the fecal-oral route and cause paralysis upon infecting the spinal cord [2]. Polio is diagnosed with certainty when the poliovirus is isolated from a patient’s stools [3]. Polio only affects humans; an effective vaccine is available, and immunity is lifelong [4]. Maintaining very high immunization coverage and enhanced AFP surveillance has helped countries in the WHO African Region [5]. Inactivated Poliovirus Vaccine (IPV) and three doses of Oral Poliovirus Vaccine (OPV) are part of the routine immunization schedule of Ghana [6].
There were 245 Wild Polio Virus type 1 (WPV1) isolates in 2020 globally, and this has reduced significantly to 6 in 2021 [6]. All the cases isolated in 2020 were reported in the Eastern Mediterranean Region, and the region reported 5 of the 6 cases reported in 2021. Failure to eradicate polio in the remaining affected countries could result in a global resurgence of the disease [7]. Circulating Vaccine-Derived Polio Virus Type 2 (cVDPV2) was also isolated (1,067 in 2020 and 659 in 2021) globally. In 2021, one case of WPV1 was isolated in the African Region (Malawi), and 530 and 521 cases of cVDPV2 were also isolated in 2020 and 2021, respectively [6].
In 1999, Ghana reported the last indigenous WPV case that caused poliomyelitis. However, 8 cases were imported into Ghana that caused an outbreak in 2003 and 2004 [8]. Ghana’s decade-long polio-free status ended in 2019 following the detection of cVDPV2. The cVDPV2 outbreaks can occur in settings with low poliovirus population immunity and cause paralysis [9]. There were 12 cases of cVDPV2 reported in 2020 and an overall total of 31 since the outbreak was declared in 2019 through Environmental Surveillance (ES) [6].
Acute Flaccid Paralysis (AFP) surveillance is the gold standard for detecting poliomyelitis. It involves the detection of enterovirus in the stool of children under 15 years [10]. Sensitivity of surveillance, completeness of reporting, case investigation and follow-up, and laboratory performance are the key indicators for AFP surveillance [10]. The certification of polio eradication regularly depends on the quality of AFP surveillance across all countries in the region, with no reported cases of Wild Poliovirus (WPV) for at least three consecutive years [11]. In contrast, polio environmental surveillance is the routine collection and examination of sewage samples to detect the presence of the virus. Environmental surveillance can identify poliovirus circulation even in the absence of proven paralytic polio cases, because paralysis only develops in 1% of poliovirus infections [12].
The AFP surveillance system in Ghana aims to detect cases of acute flaccid paralysis (AFP) and obtain laboratory confirmation of the aetiology of all suspected cases, report immediately all AFP cases using a case-based reporting form and collect at least two stool specimens (24 hours apart) from each case within 14 days. According to the WHO, Ghana was free of cVDPV2 during the assessment period but is at risk of potential outbreaks. Thus, the AFP surveillance system is critical to maintaining standards. There may be underreporting of cases due to a lack of awareness or access to healthcare facilities in certain parts of Ho municipality. We evaluated the AFP surveillance system in Ho municipality to determine if the objectives are being met and assess the usefulness and attributes.
Evaluation design and setting
The evaluation of the surveillance system was done for the period January 2017 to December 2021. The Centres for Disease Control and Prevention (CDC) Updated Technical Guidelines for Evaluating Public Health Surveillance Systems (2001) served as a guide in developing a semi-structured questionnaire/checklist for the evaluation. We interviewed stakeholders on the performance, usefulness, and attributes of the AFP surveillance system. We also reviewed the AFP case-based forms for the period to determine the indicators and data completeness for the five years. We reviewed key AFP surveillance indicators in the municipality.
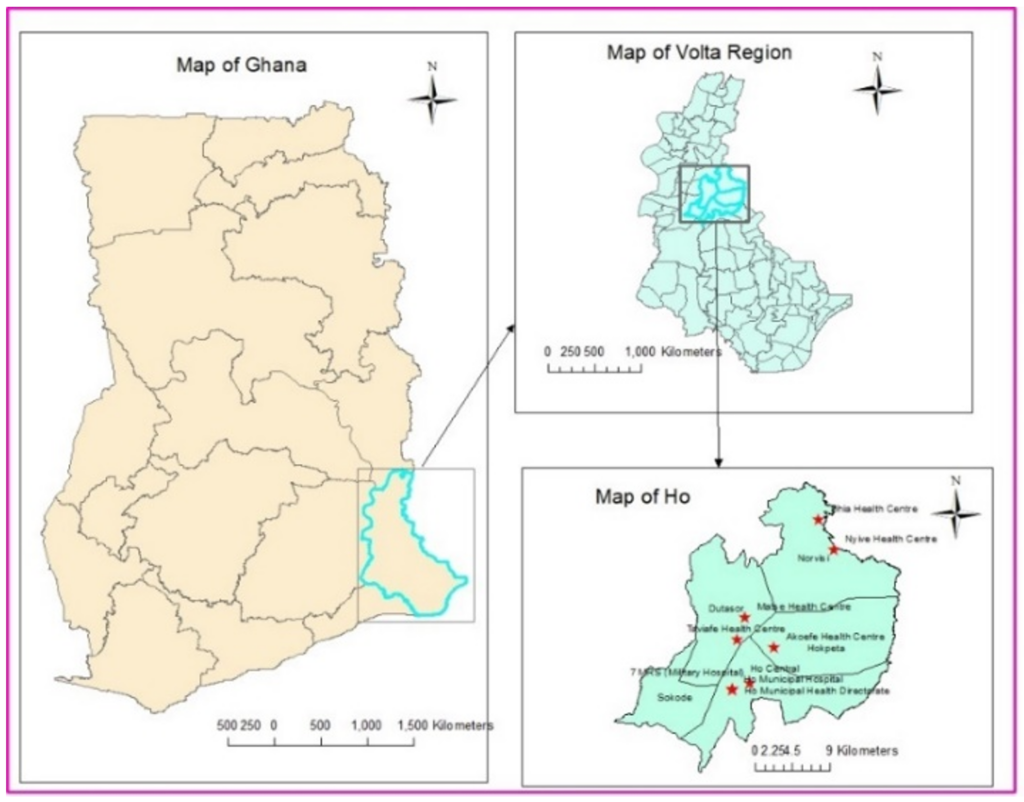
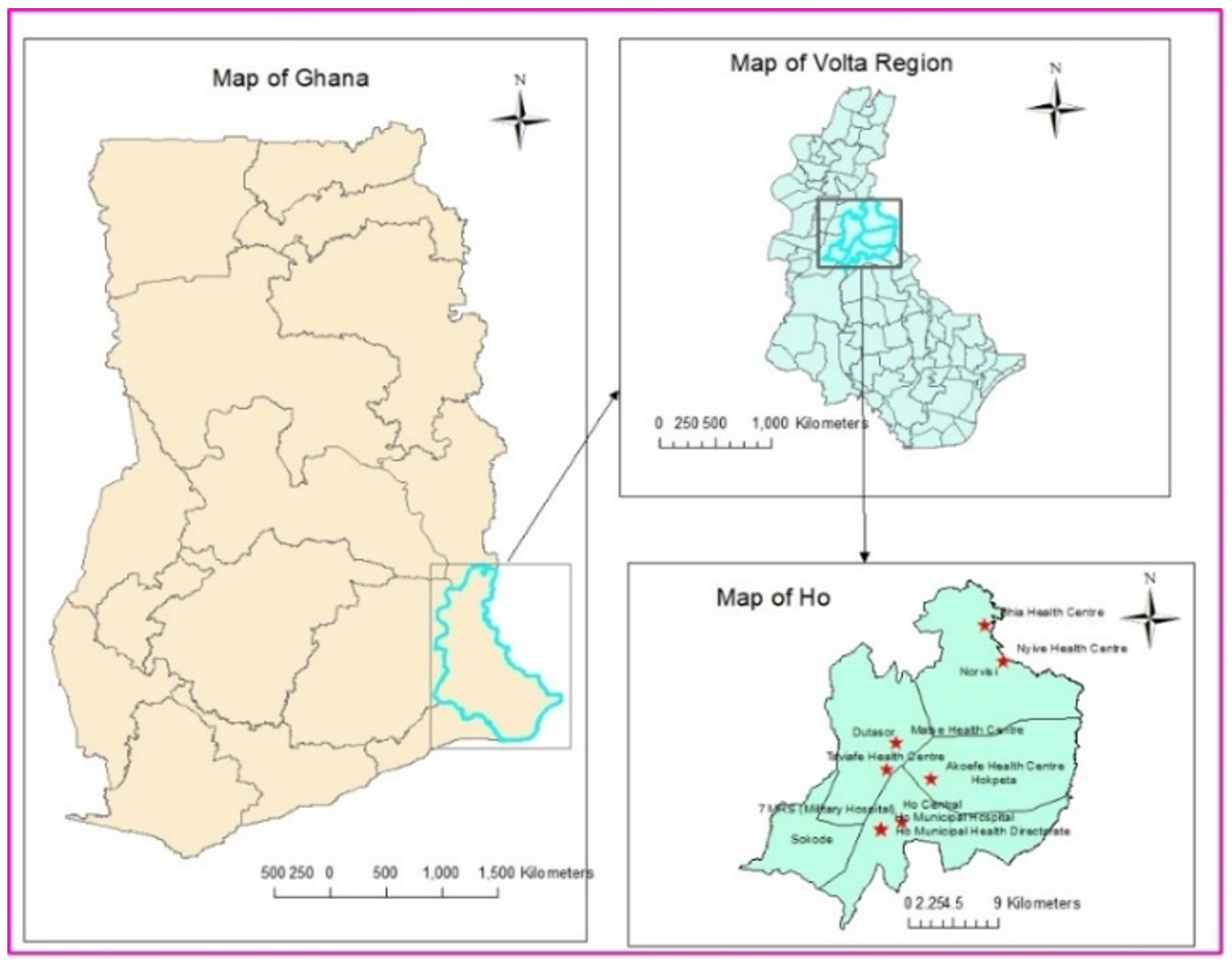
The evaluation was conducted in Ho Municipality, one of the 18 districts of the Volta Region, Ghana. The municipality has five sub-districts (Hokpeta, Norvisi, Dutasor, Sokode/Akrofu, and Ho Central) and 48 health facilities and two hospitals. All the facilities in the district offer routine immunization services. Ho municipality is bordered Northwest by the Ho West District, East and Southeast by the Adaklu-Anyigba District, and Southwest by Togo (Figure 1). Ho Municipality has a total population of 184,209 and an under-fifteen population of 96,266. The regional hospital is located in the district and receives patients from the border villages of Togo who cross to seek medical care.
Sampling techniques
We randomly selected seven health facilities in the district and at least one from each of the five districts in Ho Municipality. The health facility surveillance officers and the head of the Outpatients Department were purposively selected based on their roles in disease surveillance and patient management. In addition, staff responsible for surveillance in the Regional Health Directorate and the District Health Directorate were purposively selected due to their expertise and oversight functions. This includes the Regional Surveillance Officer, District Surveillance Officer, and District Public Health Nurse.
Operation of the system
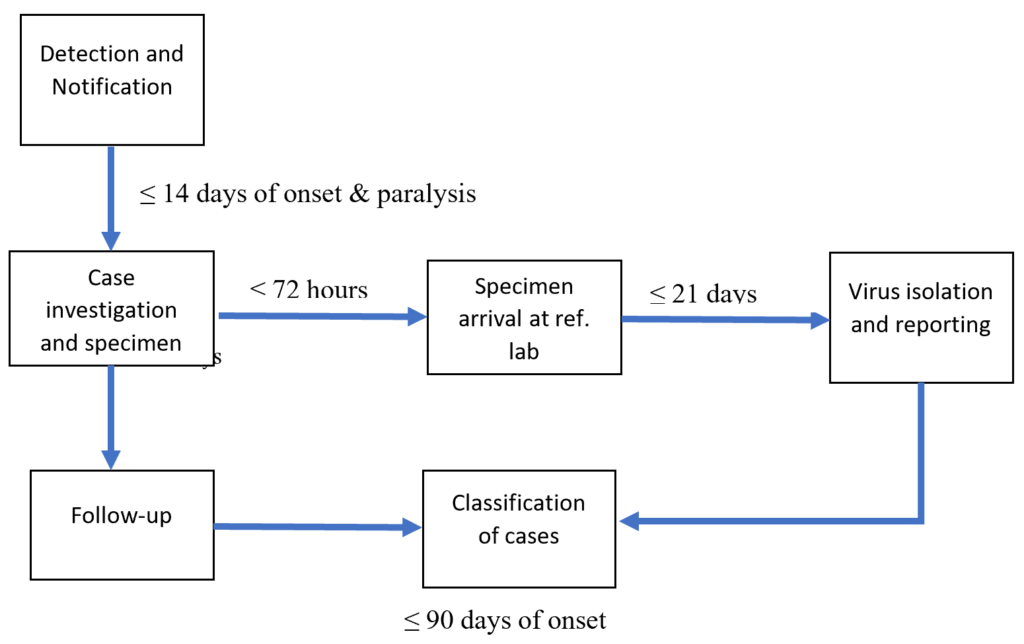
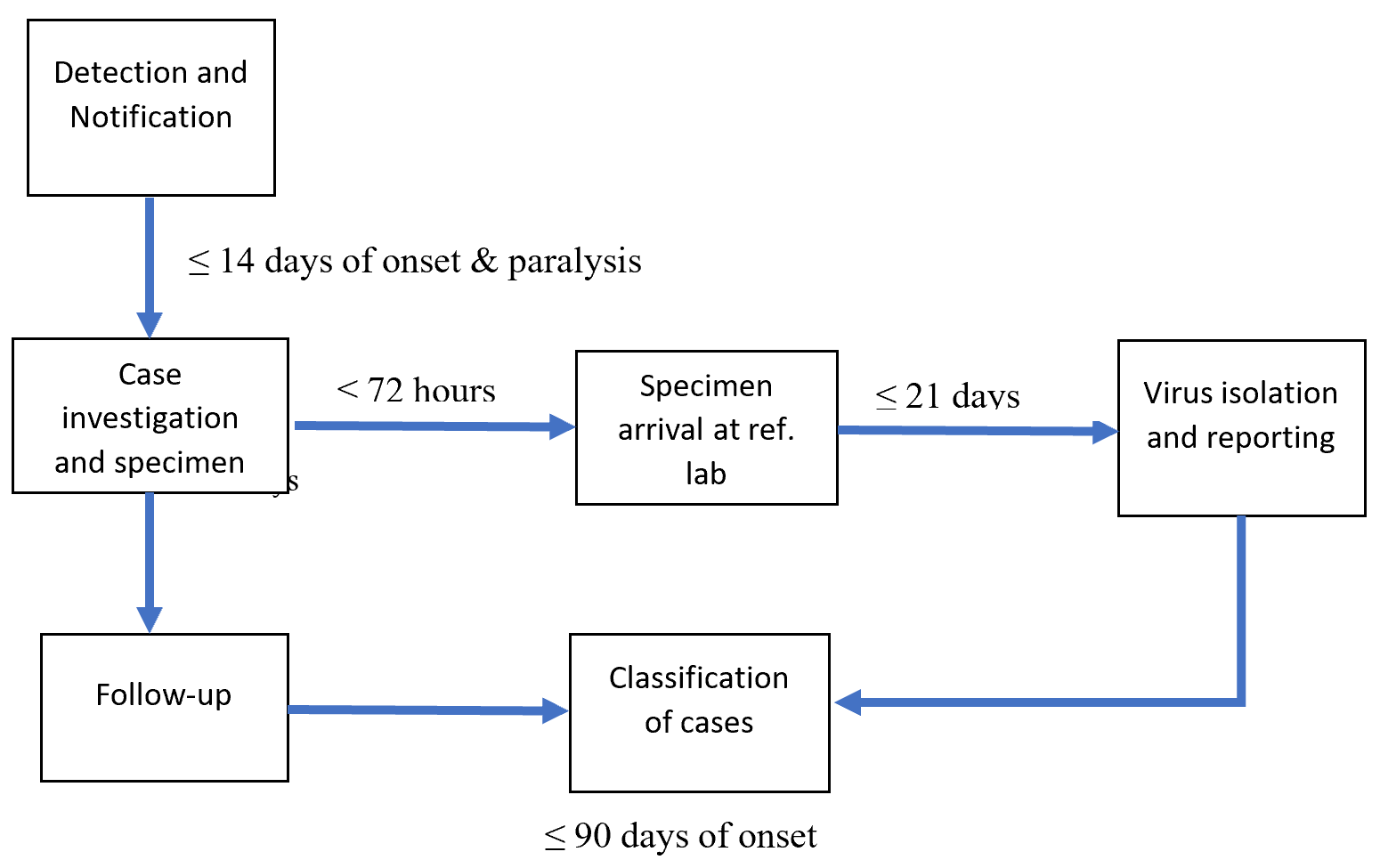
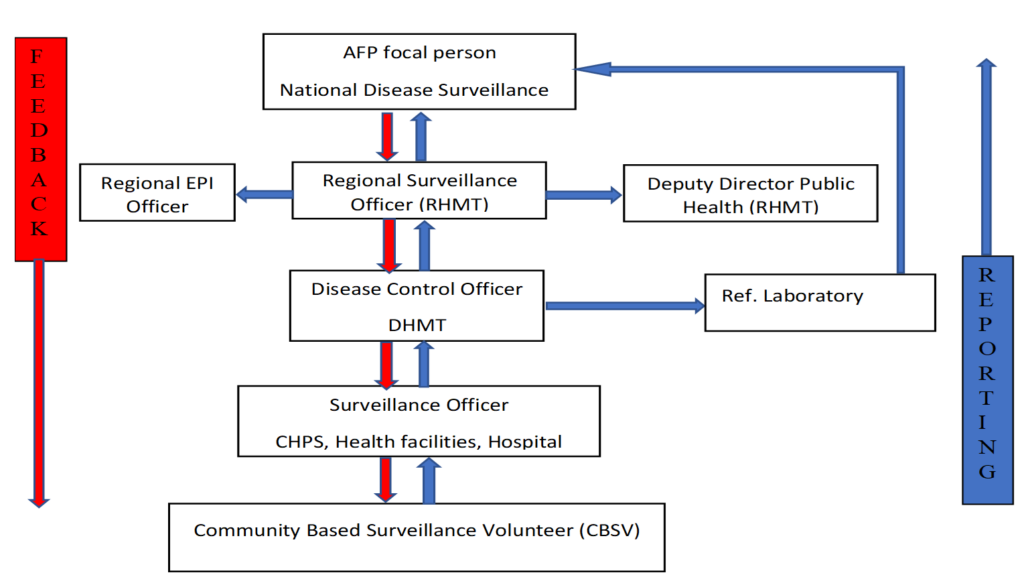
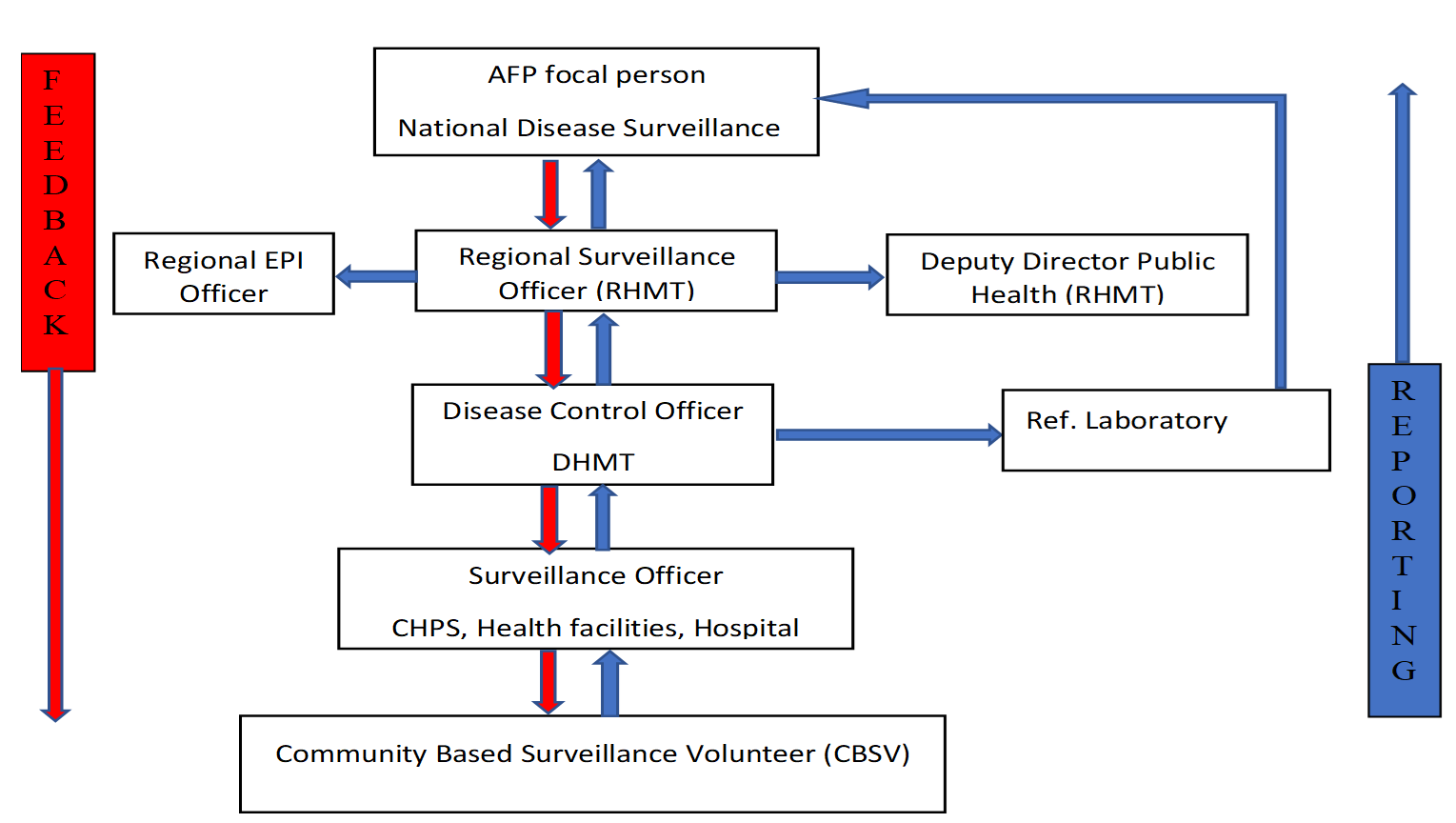
Once an AFP case is detected, two stool specimens are collected 24 – 48 hours apart and within 14 days from the onset of paralysis. The specimens are packaged using the standard triple packaging system and sent to the WHO reference laboratory within 72 hours. The results are expected within 21 days to the National AFP focal person. This result is shared with the region, district, and health facility. The stool adequacy, Sabin, and the Non-Polio Enterovirus are analysed, and a final classification is made. At 60 days, a follow-up is conducted to understand whether the case has residual paralysis (Figure 2).
Figure 3 depicts reporting and feedback on AFP surveillance in Ghana. All levels from the community to the AFP focal person at the national disease surveillance are involved. The Disease Control Officer sends specimens to the reference laboratory, and the results are shared with the AFP focal person at the national level.
Data collection
A mixed-methods design was used. A structured questionnaire was administered to 21 staff members in health facilities to capture the quantitative data. Furthermore, three key informant interviews (KII) were conducted using an interview guide to gain a deeper understanding of the perspective of the participants. We reviewed and observed surveillance tools available and verified the AFP case investigation forms in the health facilities visited. We recorded the audio of the key informants during the KII sessions. We interviewed key informants/stakeholders of the AFP surveillance system at the District Health Directorate and the Regional Health Directorate.
The system’s ability to meet its set objectives
The system’s ability to detect acute AFP cases and the availability of case-based forms (CBF) for all reported cases were evaluated. The proportion of specimens from all suspected cases sent to the laboratory and the difference in time between the first and second specimen collection were also reviewed (Table 1).
The usefulness of the system (performance)
To assess the usefulness, we considered what data generated from the system is used for and how data generated from the system influenced AFP control measures in the municipality and country at large.
Assessment of system attributes
Simplicity: The ease of the AFP case definition, the ease of filling out the Case-Based Form (CBF), and the operations of the AFP surveillance system were assessed to determine the simplicity.
Data quality: Data were reviewed to determine the completeness of the AFP data from 2017 to 2021. The data generated in the health facility, district, region, and DHIMS2 were compared based on the evaluation period. At least ≥90% of the data should be complete.
Timeliness: The time duration between two specimens collected, investigated, and reported to the next level was reviewed from filled case-based forms for the period of evaluation. The timeliness of AFP specimens to the WHO-accredited reference laboratory and the turnaround time were assessed. At least ≥90% of data should be reported on time.
Acceptability: Health facility staff were interviewed to assess their willingness to continue the AFP Surveillance System and their consistency in reporting weekly surveillance data. Community participation and the time surveillance officers are involved in AFP surveillance were also assessed. Specimens arriving in good condition, and the proportion of AFP cases that were followed for 60 days from onset, were also assessed.
Sensitivity: The Non-Polio Acute Flaccid Paralysis (NP-AFP) rate, stool adequacy, non-Polio enterovirus, timeliness of stool shipment, and stool conditions were assessed to determine the system’s sensitivity (Table 2).
Representativeness: We evaluated the participation of health facilities in AFP surveillance and reviewed reported cases by sex, age, and place.
Stability: We assessed whether services were affected by power failure and the unavailability of computers/tablets. Regional and district staff were interviewed to determine the human resources component as per their staffing norms.
Acute flaccid paralysis surveillance case definition
Suspected case: “A suspected case is defined as any child under 15 years of age with acute flaccid paralysis or any person with paralytic illness at any age in whom the clinician suspects poliomyelitis” [13].
Confirmed case: A confirmed case is defined as a suspected case with a positive laboratory result (virus isolated in the stool) [7]
Data analysis
Quantitative data were presented using frequencies and tables. We calculated the AFP performance indicators and analysed them in terms of rates and proportions. Qualitative data were recorded and later transcribed to narrate the operations of the AFP surveillance system, its procedures, and the reporting flow of the AFP surveillance in Ghana to assess its simplicity. We quoted a few responses for qualitative attributes.
Ethical statement
The Head of the Diseases Surveillance Department of the Ghana Health Service granted permission to conduct the evaluation. Permission was obtained from the regional and district directorates and health facilities before the start of the evaluation. All respondents were provided with the information sheet, and written consent was obtained. They were assured of their confidentiality. Data was kept on password-protected devices and made available only on a need-to-know basis.
A total of seven health centers were visited. The evaluation recruited 21 health workers, amongst whom, more than half of the respondents, 52.4% (11/21), were nurses, and 28.5% (6/21) were Disease Control Officers. The majority, 61.9% (13/21), were females, and most of the participants, 57.1% (12/21), were between the ages of 20 and 30 years. The mean age of the participants was 31.9 ±6.5 years (Table 2).
The system’s ability to meet its set objectives
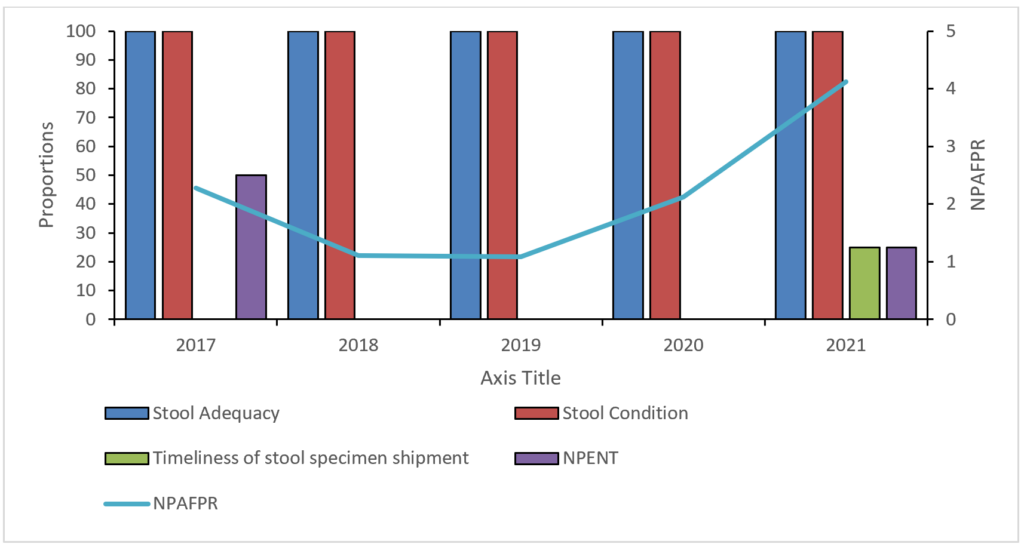
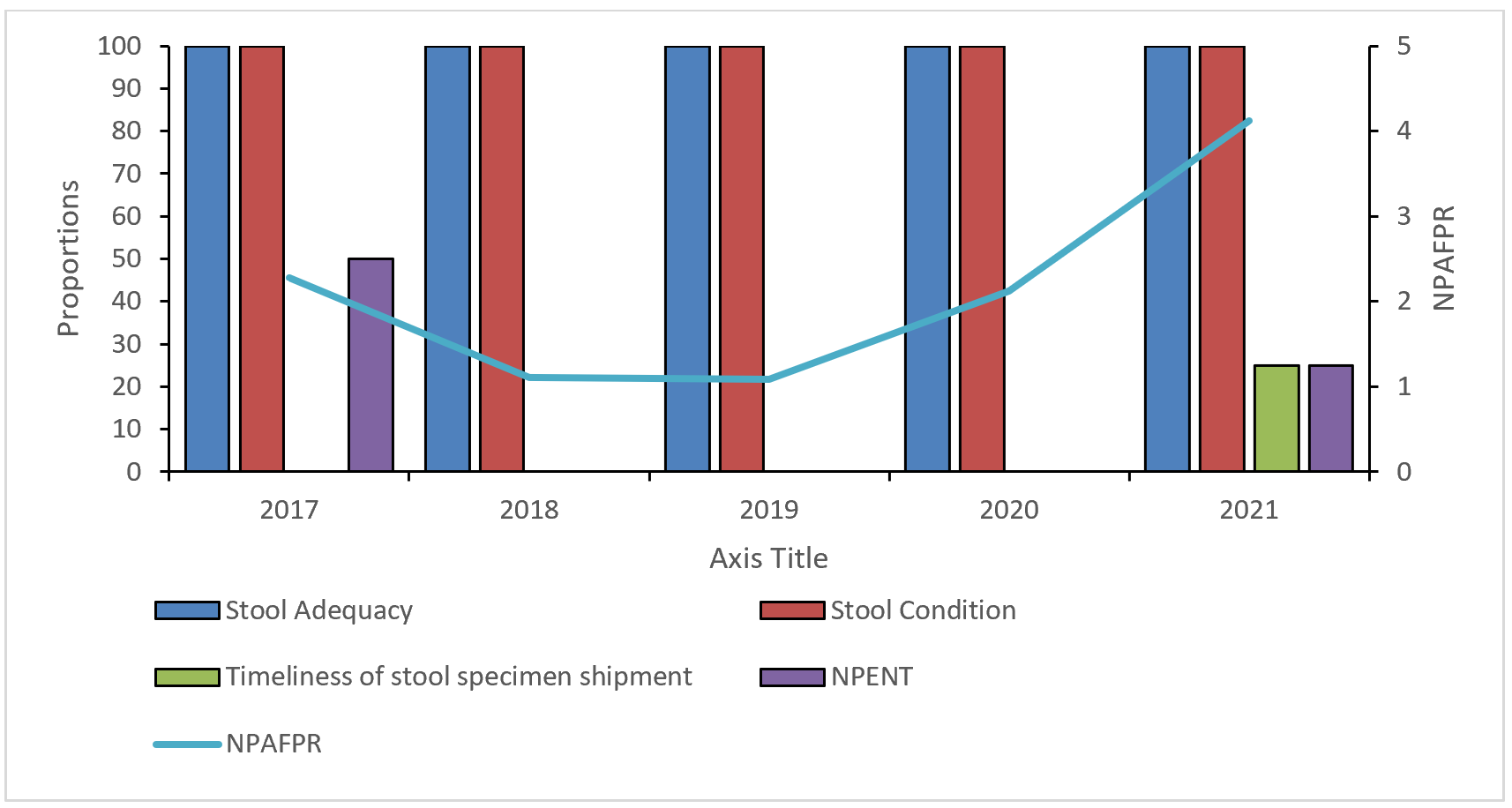
During the five years, the district reported at least 1 case each year, although it had not met the NP-AFP rate of 2 per 100,000 in 2018 and 2019. The district recorded 1.11 per 100,000 and 1.09 per 100,000 populations in 2018 and 2019, respectively (Figure 4). However, the laboratory results were not available in the district, and feedback comes in 2 to 6 months after the sample is taken to the laboratory. The case-based forms of all the cases reported were available at the district. All the cases were investigated and notified immediately. Two stool specimens were collected within 24 – 48 hours apart from all the AFP cases reported during the evaluation period.
The usefulness of the system (performance)
The region and the district monitor the trend graph of AFP cases. Though they had a meeting, no minutes were available. It was highlighted that in the last quarter of 2021, the municipality, with the support of district and regional staff, embarked on an active case search funded by the World Health Organization to meet the NP-AFP rate target.
Attributes of the AFP surveillance system
Simplicity: Most participants (13; 61.9%) knew the case definition, and 4 (19.5%) had previously identified a case and completed the case-based form. It takes 21 days before the polio virus is isolated and reported. All the participants highlighted the ease of filling out the case investigation form.
Flexibility: The AFP reporting form was modified from 44 variables to 75 variables. Among the respondents, 81.0% (17/21) said that the changes have not disrupted the smooth operations of the surveillance system. More than three-quarters, 90.5% (19/21) of the respondents had used the electronic database to report.
Data quality: The number of AFP cases reported by the district, the data shown in the region and the DHIMS2 were 100% accurate. However, the completeness of the variables filled in the CBF reported from 2017 to 2021 was 68.04% (Table 3).
Timeliness: All the reported cases were investigated on time, and stool specimens from the cases were collected 24-48 hours apart and within 14 days (Table 3). Ninety percent (9/10) of the specimens sent to the reference laboratory were sent after 72 hours of collection (Table 4).
Sensitivity: The non-Polio AFP rate per 100,000 was less than the targets in 2018 (1.11/100,000), 2019 (1.09/100,000), and 2020 (2.12/100,000). The average NP-AFP was 2.14 per 100,000 with a minimum of 1.09 and a maximum of 4.12 per 100,000 population under 15 years. The non-polio enterovirus (NPENT) detection rate was 0% from 2018 to 2022. Overall, only 20% (2/10) had non-polio enterovirus in the stool (Figure 4).
Acceptability: All the facilities visited are willing to continue AFP surveillance, albeit more than half of the respondents 12 (57.1%) lack support in their day-to-day activities. All 7 facilities reported weekly and recorded 100% timeliness. The proportion of specimens arriving at the laboratory in good condition was 100% across the five years, except in 2021, which recorded 75%.
All cases were investigated within 48 hours, but only one specimen was sent to the reference laboratory within the required 72-hour deadline. All the cases were discarded, and there were only three cases that were followed up (2 cases in 2017 and 1 case in 2020), 60 days after the onset of the paralysis.
One of the stakeholders highlighted that “staff lack motivation to partake in surveillance and most of them do not read books to broaden their scope”. Community participation in the urban areas was poor as opposed to the rural communities. Almost all participants, 20 (95.2%), believe that community participation is moderate.
Representativeness: All the health facilities in the district participate in AFP surveillance. Cases were reported from both males (4) and females (6), and 70% were under five years (Table 5). However, the 10 reported cases for the five years came from only two sub-districts, i.e., Norvisi and Ho Central.
Stability: “High staff attrition and inadequate specimen collection tools are a challenge in Ho Municipality” (Staff RHMT). All the facilities visited have either functional computers or tablets to enter routine surveillance data in the DHIMS2. All the facilities visited displayed a copy of the case definition at the outpatient.
This study evaluated the AFP surveillance system in Ho municipality to determine if the objectives are being met and assess the attributes and usefulness. More than half of the cases were female, and the children were less than five years old. More than three-quarters had at least a dose of the oral polio vaccine. We found that two stool specimens were collected within 24 – 48 hours apart and within 14 days of all the AFP cases reported during the evaluation period. Our study also provides evidence that feedback on the laboratory results of the cases was never available within the expected 21-day period. There is a delay in sample transportation from the district to the WHO-accredited laboratory.
The finding that most reported AFP cases were among children aged <5 years is significant and suggests that WPV or cVDPV could have been detected, since poliomyelitis mainly affects children within this age group[14]. Similarly, other studies evaluating AFP surveillance systems found that most AFP cases were among children under 5 years old in Kenya [14] and Jordan [15]. The Volta Region met the NP-AFP targets in 2018 and 2019 [16], but the Ho Municipality district did not meet the target. A similar finding was observed in Kenya, where progress has been made at the national level, but a declining trend has been observed in some other regions [14].
Anecdotal reports from surveillance personnel suggest that most supervisors do not support silent districts in meeting their NPAFP rate once regional targets are met. The average Non-Polio Acute Flaccid Paralysis (NP-AFP) rate was lower than the study in Northern Sudan, which reported 4/100,000 under 15 population [17]. The findings are comparable to the study conducted in South Sudan, with a minimum and maximum rate of 1.2 to 4.4 per 100,000 under-15 population, respectively [18]. Failure to meet the NPAFP rate in those years could be due to inadequate numbers of surveillance officers to conduct active case searches in the community and limited community engagement. Community Health Workers are crucial in polio surveillance once properly oriented and actively engaged. High staff attrition and inadequate specimen collection tools have compromised the stability of the surveillance system in the district.
We found that the surveillance system was useful, and the district staff were entirely responsible for monitoring trends. However, meeting minutes were not available at the District Health Office to document discussions, decision-making, and actions taken regarding AFP surveillance. Similar study findings have been observed in Mashonaland West Province [1], where the surveillance system was perceived as useful, and health workers are more likely to participate diligently. However, failure to produce meeting minutes is purportedly an indication that the meeting was probably not held.
In addition, the findings showed that the AFP surveillance system was complex, and all the facilities visited had a case definition displayed on the wall in the OPD department. It takes precisely 21 days for an AFP specimen to be processed, and the National Polio Expert Committee must meet to classify cases. In addition, all the health facilities visited did not have a single unfilled AFP Case Base Form and had no idea how to fill out the form. There is a knowledge gap among the health workers, and they had to rely on the District Surveillance Officer to fill in the AFP CBF and sample collections. These findings were not in conformity with a study in Nigeria, which reported that the AFP surveillance system is simple due to the ease of filling out forms and the straightforward case definition [19]. All specimens were collected within 24-48 hours; however, specimens were not transported to the reference laboratory promptly. A similar finding was reported in the Mwenezi district, Masvingo [20]. This could be because of the distance from the laboratory and the logistics involved in sending the specimens. A delay in sending specimens can reduce the chances of isolating the polio virus from the stool.
We found that the data completeness was lower than the 97% data completeness of a study conducted in Kebbi State, Nigeria [19]. The lack of feedback on laboratory results for cases to complete the outcome of the AFP case on the CBF was one of the missing variables. The date specimen sent to the lab is also often missing in some of the cases reported. This could also mean that the specimen was not sent to a laboratory for processing. Regular supervision from a higher level will evidently improve the data completeness.
We found that the sex distribution of AFP cases was higher among females. The finding is not in conformity with a study in Jordan and Sudan that found that more cases were males, respectively [17] [15]. However, the differences were minute, and all sexes had equal exposures to AFP. Most of the cases were under five years and corroborate the study in Sotoko State, Nigeria [21] [22], where 82,4% of cases were below five years. Predictive value positive (PVP) is defined as “the proportion of reported cases that have the health-related event under surveillance” [21]. It is difficult to determine PVP for AFP surveillance in Ghana, as the diagnosis is strictly clinical and only the true AFP cases are reported.
Our study has some limitations. The study participants were relatively small. This limits the generalizability of the findings. However, the purposive inclusion of staff directly involved in AFP surveillance at all levels enhances the credibility and relevance of the findings for program improvement in Ho municipality. In addition, cumulative data from all the health facilities in the district were used during the review.
The AFP surveillance system in Ho municipality is partially meeting its objectives. It is useful, partially stable, and partially sensitive. The system is acceptable, representative, and flexible, but has poor data quality and timeliness. We recommend that the District Health Directorate strengthen the AFP case surveillance system, such as capacity strengthening among health workers and community volunteers, active case search in the community, improve timeliness of sample transportation to the WHO-accredited laboratory, strengthen community participation, and increase public awareness and cooperation in AFP case surveillance.
What is already known about the topic
What this study adds
The authors of this work declare no competing interests. Delia Bandoh is an Associate Editor at the Journal of Interventional Epidemiology and Public Health (JIEPH) and a co-author of this manuscript. In line with the journal’s conflict of interest policy, she was fully recused from the peer review process and had no involvement in editorial handling or decision-making for this submission. An independent editor oversaw the review and decision-making process.
I acknowledge the Ghana Field Epidemiology and Laboratory Training Program and the Ghana Health Services for their immense support during the one-day field training. Special thanks go to the Regional Health Directorate of the Volta Region and the District Health Management of Ho Municipality, Ghana, for permitting us the AFP surveillance system in Ho District.
Conceptualization: Bakalilu Kijera, Abdul Nasir Alhasan
Data Collection: Bakalilu Kijera, Sarja Jarjusey, Mary Bobb, Lamin F Manjang
Methodology: Bakalilu Kijera, Abdul Nasir Alhasan
Formal analysis: Bakalilu Kijera, Abdul Nasir Alhasan
Resources: Bakalilu Kijera, Abdul Nasir Alhasan, Sarja Jarjusey, Mary Bobb, Lamin F Manjang, Donne Ameme, Charles Lwanga Noora, Delia Bandoh, Ernest Kenu
Supervision: Abdul Nasir Alhasan, Donne Ameme, Charles Lwanga Noora, Delia Bandoh, Ernest Kenu
Writing – original draft: Bakalilu Kijera
Writing – review & editing: Bakalilu Kijera, Abdul Nasir Alhasan, Sarja Jarjusey, Mary Bobb, Lamin F Manjang, Donne Ameme, Charles Lwanga Noora, Delia Bandoh1, Ernest Kenu
Manuscript writing: Bakalilu Kijera
| Indicator | Numerator | Denominator | Target |
|---|---|---|---|
| Non-polio AFP rate | # Cases discarded as NPFPR in children aged <15 | # Population aged <15 years | ≥2 |
| Stool adequacy | # of 2 stool specimens collected ≥24 hours apart, within ≤14 days of onset of paralysis | # AFP cases | ≥80% |
| Stool Condition | # AFP cases with two stools that arrived in good condition at the WHO-accredited lab | # AFP cases | ≥80% |
| Non-Polio Enterovirus | # of AFP cases with enterovirus | # AFP cases | ≥10% |
| Timeliness of Investigation | # AFP cases with ≤48 hours between notification and investigation | # AFP cases | ≥80% |
| Timeliness of stool specimen shipment | # AFP cases with ≤3 days between stool collection and arrival at the WHO-accredited lab | # AFP cases | ≥80% |
| Characteristics | Frequency (%) |
|---|---|
| Sex | |
| Male | 8 (38.1) |
| Female | 13 (61.9) |
| Age | |
| 20-30 | 12 (57.1) |
| 31-40 | 8 (38.1) |
| Above 40 | 1 (4.8) |
| Designation | |
| Disease Control Officer | 6 (28.5) |
| Nurse | 11 (52.4) |
| Physician Assistant | 1 (4.8) |
| Field assistant | 2 (9.5) |
| Public Health Nurse | 1 (4.8) |
| Name of Case-Based Form | # Of variables | # Of variable properly filled | # Of missing variable | # Of improperly filled variable | Completeness (%) |
|---|---|---|---|---|---|
| GHA-VOL-HOV-017-001 | 44 | 32 | 12 | 0 | 72.7 |
| GHA-VOL-HOV-017-002 | 44 | 32 | 12 | 0 | 72.7 |
| GHA-VOL-HOV-018-001 | 44 | 32 | 12 | 0 | 72.7 |
| GHA-VOL-HOV-019-001 | 75 | 50 | 25 | 0 | 66.6 |
| GHA-VOL-HOV-2020-001 | 75 | 50 | 25 | 0 | 66.6 |
| GHA-VOL-HOV-2020-002 | 75 | 50 | 25 | 0 | 66.6 |
| GHA-VOL-HOV-2021-001 | 75 | 50 | 25 | 0 | 66.6 |
| GHA-VOL-HOV-2021-002 | 75 | 49 | 26 | 0 | 65.3 |
| GHA-VOL-HOV-2021-003 | 75 | 49 | 26 | 0 | 65.3 |
| GHA-VOL-HOV-2021-004 | 75 | 49 | 26 | 0 | 65.3 |
| Overall | 68.04 | ||||
| Case-Based Form | Specimens collected 24-48 hrs apart | Specimen sent to the Ref lab |
|---|---|---|
| GHA-VOL-HOV-017-001 | T | L |
| GHA-VOL-HOV-017-002 | T | L |
| GHA-VOL-HOV-018-001 | T | L |
| GHA-VOL-HOV-019-001 | T | L |
| GHA-VOL-HOV-2020-001 | T | L |
| GHA-VOL-HOV-2020-002 | T | L |
| GHA-VOL-HOV-2021-001 | T | NR |
| GHA-VOL-HOV-2021-002 | T | NR |
| GHA-VOL-HOV-2021-003 | T | NR |
| GHA-VOL-HOV-2021-004 | T | T |
| Overall Timeliness (%) | 100% | 10% |
T= Timely, L = Late, NR= Not recorded
| Variable | Value, n (%) |
|---|---|
| Sex | |
| Male | 4 (40) |
| Female | 6 (60) |
| Age (years) | |
| <5 | 7 (70) |
| 5-10 | 2 (20) |
| >10 | 1 (10) |
| Vaccination status (OPV doses) | |
| 1-3 | 4 (40) |
| ≥4 | 4 (40) |
| Unknown | 2 (20) |
| Clinical characteristics | |
| Fever | 3 (23.1) |
| Asymmetric paralysis | 1 (7.7) |
| Rapid progression of paralysis | 9 (69.2) |