Outbreak Investigation | Open Access | Volume 9 (2): Article 94 | Published: 04 June 2026

Views: 690
Menu, Tables and Figures
| Variable | Cases (%) | Controls (%) | p-value |
|---|---|---|---|
| Sex | |||
| Male | 69 (95.8) | 63 (87.5) | 0.07 |
| Female | 3 (4.2) | 9 (12.5) | 0.70 |
| Age (Years) | |||
| ≤10 | 1 (1.4) | 0 (0.0) | 0.31 |
| 11-20 | 6 (8.3) | 5 (6.9) | 0.75 |
| 21-30 | 36 (50.0) | 31 (43.0) | 0.40 |
| 31-40 | 22 (30.6) | 29 (40.3) | 0.22 |
| 41-50 | 6 (8.3) | 4 (5.7) | 0.50 |
| >50 | 1 (1.4) | 3 (4.1) | 0.31 |
| Median age (IQR) | 28(23-36) | 30(25-36) | |
| Level of education | |||
| Secondary | 53 (73.6) | 52 (72.2) | 0.84 |
| Primary | 17 (23.6) | 19 (26.4) | 0.76 |
| Up to grade 6 | 2 (2.8) | 0 (0.0) | 0.15 |
| Never went to school | 0 (0.0) | 1 (1.4) | 0.31 |
| Occupation | |||
| Artisanal miner | 51 (70.8) | 64 (88.9) | 0.84 |
| Farmer | 8 (11.1) | 1 (1.4) | 0.05 |
| Vendor | 6 (8.3) | 2 (2.7) | 0.14 |
| Fisherman | 3 (4.2) | 0 (0.0) | 0.08 |
| *IQR: Interquartile Range | |||
Table 1: Demographics Characteristics of Respondents, Ward 13, Mhondoro Ngezi District 2022
| Variable | Cases n=72(%) | Controls n=72(%) | Odds Ratio | 95% CI | p-value |
|---|---|---|---|---|---|
| Sex: | |||||
| Female | 3 (4.2) | 9 (12.5) | 0.3 | 0.07 — 1.17 | 0.12 |
| Male | 69 (95.8) | 63 (87.5) | |||
| Age (Years): | |||||
| ≥20 | 65 (90.3) | 66 (92.9) | 0.7 | 0.17 — 2.73 | 0.76 |
| <20 | 7 (9.8) | 5 (7.1) | |||
| Occupation: | |||||
| Artisanal miner | 51 (70.8) | 50 (69.4) | 1.06 | 0.51 — 2.18 | 0.85 |
| Other | 21 (26.4) | 22 (30.6) | |||
| History of travel to malarias area | |||||
| Yes | 6 (8.3) | 5 (6.9) | 1.2 | 0.3 — 5.3 | 0.5 |
| No | 66 (9.7) | 67 (93.1) | |||
| Sleeping in properly constructed house | |||||
| Yes | 9 (12.5) | 28 (38.9) | 0.2 | 0.09 — 0.55 | 0.01 |
| No | 63 (87.5) | 44 (61.1) | |||
| Sleeping outside | |||||
| Yes | 57 | 23 | 8.09 | 2.06 — 9.4 | 0.01 |
| No | 15 | 49 | |||
| Stagnant water near sleeping area | |||||
| Yes | 58 (80.6) | 47 (65.3) | 2.2 | 1.03 — 4.7 | 0.03 |
| No | 14 (19.4) | 25 (34.7) | |||
| Permanent resident in Ward 13 | |||||
| Yes | 44 (61.1) | 12 (16.7) | 7.8 | 3.6 — 17.1 | 0.01 |
| No | 28 (38.9) | 60 (83.3) | |||
| Outdoor activities at night | |||||
| Yes | 51 (70.8) | 47 (65.2) | 1.2 | 0.63 — 2.6 | 0.47 |
| No | 21 (29.2) | 25 (34.8) | |||
| Tall grass and vegetation around sleeping area | |||||
| Yes | 64 (88.9) | 67 (93.1) | 1.67 | 0.45-6.84 | 0.28 |
| No | 8 (11.1) | 5 (6.9) | |||
| Owning ITNSs | |||||
| Yes | 6 (8.30 | 25 (34.7) | 0.17 | 0.05 — 0.47 | 0.01 |
| No | 66 (91.7) | 47 (65.3) | |||
| Use of ITNSs | |||||
| Yes | 8 (11.1) | 25 (34.7) | 0.23 | 0.08 — 0.6 | 0.01 |
| No | 64 (88.9) | 47 (63.5) | |||
| ITNSs available at all sleeping places | |||||
| Yes | 7 (9.7) | 26 (36.1) | 0.19 | 0.06 — 0.5 | 0.01 |
| No | 65 (90.3) | 46 (63.9) | |||
| Wearing unprotective clothing | |||||
| Yes | 57 (79.2) | 60 (88.3) | 1.31 | 0.56 — 3.05 | 0.52 |
| No | 15 (20.8) | 12 (16.7) |
Table 2: Bi-variate analysis for contracting malaria, Ward 13, Mhondoro Ngezi District 2022
| Variable | OR | AOR | 95% CI | p-value |
|---|---|---|---|---|
| Permanent residence in ward 13 | 7.8 | 9.7 | 4 — 23.7 | 0.01 |
| Sleeping outside | 4.4 | 4.7 | 4.7 — 12.4 | 0.01 |
| Stagnant water near sleeping area | 2.2 | 3.7 | 1.4 — 9.6 | 0.01 |
Table 3: Independent factors associated with contracting malaria, Ward 13 Mhondoro Ngezi 2022
Derek Masokovere1,&, Daniel Chirundu2, Gerald Shambira1, Tsitsi Patience Juru1, Notion Tafara Gombe1, Mufuta Tshimanga1
1Department of Primary Health Care Sciences: Family Medicine, Global and Public Health Unit, University of Zimbabwe, Harare, Zimbabwe, 2Kadoma City Health Department, Kadoma, Zimbabwe
&Corresponding author: Derek Masokovere, Department of Primary Health Care Sciences: Family Medicine, Global and Public Health Unit, University of Zimbabwe, Harare, Zimbabwe, Email: dmasokovere@gmail.com ORCID: https://orcid.org/0000-0003-0300-1239
Received: 03 Jan 2026, Accepted: 26 May 2026, Published: 04 Jun 2026
Domain: Infectious Disease Epidemiology
Keywords: Mhondoro-Ngezi, Malaria resurgence
©Derek Masokovere et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Derek Masokovere et al. Resurgence of Malaria, Ward 13, Mhondoro-Ngezi, Zimbabwe, 2022. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):94. https://doi.org/10.37432/jieph-d-26-00005
Introduction: Mhondoro-Ngezi district is in the malaria elimination phase. However, Ward 13 experienced an unusual increase in malaria cases, surpassing the action threshold from week 11 to week 22 of 2022. Enhanced case-based surveillance was ongoing. We investigated the outbreak to determine factors associated with the resurgence of malaria in Ward 13, Mhondoro-Ngezi district, 2022.
Methods: We conducted an unmatched 1:1 case-control study. A case was any resident of Ward 13 who presented with headache, fever, general body malaise, joint weakness, vomiting and tested positive for a rapid diagnostic test from 24 February to 7 April 2022. We collected data using a pre-tested, interviewer-administered questionnaire. Data were analysed using Epi Info 7.
Results: We interviewed 72 cases and 72 controls. Males were 69 (95.8%) among cases and 63 (87.5%) among controls (p=0.07). The median age for cases was 28 years (IQR: 23-36) and 30 years (IQR: 25-36) for controls. Factors that were significantly associated with contracting malaria were stagnant water bodies near sleeping home (OR=2.2; 95%CI: 1.03-4.7), being a permanent resident of ward 13 (OR=7.8; 95%CI: 3.6-17.1) and sleeping outside at night (OR=8.09; 95% CI: 2.06-7.1). Significant factors associated with the reduction of malaria transmission were sleeping in a house with closable windows and openings (OR=0.2; 95%CI: 0.09 – 0.55) and residing outside Ward 13.
Conclusion: Sleeping near a stagnant water source, being a permanent resident of Ward 13 and sleeping outside at night increased malaria transmission. Sleeping under an ITN and in a house with closable windows reduced malaria transmission. We recommended the distribution of ITNs.
Malaria is a life-threatening disease caused by protozoan parasites of the genus Plasmodium. Globally, an estimated 241 million malaria cases were reported in 2020. There was an estimated increase of 13 million cases from 227 million in 2019. Most of this increase came from the WHO African Region [1]. Malaria is the 4th leading cause of preventable morbidity and mortality in Africa. A total of six Sub-Saharan African countries accounted for about 55% of all cases globally in 2020 [2].
The major malaria transmission season in Zimbabwe occurs during the rainy season between November and April, with the average temperature ranging between 180 and 30 0 Celsius. Malaria is a major public health problem affecting all age groups in Zimbabwe[3]. P. falciparum has been the predominant malaria parasite, causing 98% of all reported malaria cases. Approximately 1 in 12 children in Zimbabwe dies before their 5th birthday due to malaria[4].
The national malaria control program (NMCP) in Zimbabwe classifies districts into control and elimination activities based on incidence. Districts with a malaria incidence of less than 5 per 1000 population are classified into elimination, while districts with a malaria incidence ≥5 per 1000 population are classified into control. Mhondoro-Ngezi district is non-malaria endemic and is one of the 28 districts in Zimbabwe implementing malaria elimination activities. The district managed to reduce malaria incidence to less than 5 per 1000 population [5]. In 2017, the incidence further decreased to less than 2 per 1000 population. The district was certified malaria-free in 2019 by the Zimbabwe National Malaria Control Program [6]. Certification came after the district maintained an incidence of less than 2 per 1000 population from 2017 to 2019.
Battlefields (Ward 13) in Mhondoro-Ngezi District experienced an unusual increase in malaria cases of over 1000% from 14 March 2022 (Week 11). Malaria cases surpassed the action threshold of two cases to 41 cases in the month of March alone and continued to increase each week. This was despite all the other wards in Mhondoro-Ngezi district reporting malaria cases that were below the threshold limit. The district has, in previous years, successfully managed to reduce the malaria incidence to less than 2 per1000 population. This was achieved through enhanced case surveillance of positive local malaria cases, risk communication and community engagement and case management. Despite ongoing implementation of these interventions, in 2022, malaria cases continued to surpass the action threshold.
We investigated the malaria outbreak to determine the factors associated with the resurgence of malaria cases and transmission in Ward 13, Mhondoro-Ngezi district and to come up with tailor-made prevention and control strategies that will harness epidemics in the future. Investigating this outbreak further assisted in coming up with interventions that led to the reduction of malaria morbidity in Ward 13, Mhondoro-Ngezi district, 2022.
Study setting
The study setting was Mhondoro-Ngezi District (Ward 13), which is located about 30km south of Kadoma City along the Harare-Bulawayo highway. Ward 13 has an estimated population of 21,304 according to ZimStat 2012 projected population estimates. Males are 9,093, and females are 12,211. Children under 5 years are 2 813. The main economic activities in this area are artisanal mining, subsistence agriculture and fishmongering. Malaria transmission is high in the Magirasi area, where artisanal mining is the main economic activity. There are two health facilities in the Ward, which are Battlefields Clinic and Battlefields 5 Brigade Clinic. ZNA Battlefields 5 brigade clinic caters mostly for members of the Zimbabwe National Army staying at the camp.
Study design and population
We conducted an unmatched 1:1 case-control study. A case was defined as any resident of Ward 13, Mhondoro Ngezi district, who presented with headache, fever, general body malaise, joint weakness and tested positive for a rapid diagnostic test (RDT) from 24 February to 7 April 2022. A control was defined as any resident of ward 13, Mhondoro Ngezi district, who tested negative for an RDT test from 24 February to 7 April 2022.
The study population were residents of Ward 13, Mhondoro Ngezi district. The District Medical Officer (DMO), District Environmental Health Officer (DEHO), District Nursing Officer (DNO) and the District Pharmacy Manager (DPM) were key informants. The study unit was an individual resident of Ward 13 who was tested for malaria using RDT.
Inclusion and exclusion criteria
Inclusion criteria were any resident of ward 13, Mhondoro Ngezi district, who was tested by RDT from 24 February to 7 April 2022 and consented to participate in the study. The exclusion criteria were any resident of ward 13, Mhondoro Ngezi, who was tested by RDT and did not consent to participate in the study or was seriously ill.
Sampling frame
The sampling frame was the RDT register for malaria. The line list could not be used as a sampling frame since it contained positive cases only
Sample size calculation
Sample size was calculated using Stat Calc function in Epi-Info 7™ based on a study by Masango et.al. (2019) on factors associated with malaria transmission in Mudzi district [7]. Assuming engaging in outdoor activity at night was a risk factor for contracting malaria with an odds ratio of 6.3 at 95% confidence interval using 80% power, the calculated minimum sample size was 72 cases and 72 controls.
Sampling
We selected cases and controls from the RDT register using simple random sampling. Cases and controls from the RDT register were allocated numbers. The lottery system was used to separately select cases and controls using the numbers. Key informants were purposively selected.
Data collection
We collected data from participants using a pre-tested interviewer-administered questionnaire to capture demographic data, risk factors of contracting malaria, health-seeking behaviours and risky behaviours. Clinical records were reviewed. An interview guide was used to collect data from key informants. A checklist was used to assess environmental factors as well as outbreak preparedness and response.
Collection of adult mosquitoes was done using pyrethrum spray catches and prokopakTM aspirator as described by Sande et. al. (2015)[8]. Harvesting of larvae and larval source management was also conducted as described by Zengenene et. al. (2022)[4]. Data on malaria were collected using microscopy as described by Takarinda et. al. (2022)[9]. Thick and thin blood slides were prepared and examined under the microscope for all the cases.
Data capture and analysis
Data were captured using Epi Info 7™ (CDC) ver. 7.2.4.0. The software was used to generate frequencies, proportions, and medians. Univariate and bivariate analyses were conducted using Epi Info 7™ (CDC) ver. 7.2.4.0. Backward logistics regression analysis was performed on variables that are significant at p≤0.25. Microsoft Excel™ was used to generate the epidemic curve. Google Earth™ software was used to generate a spot map. A checklist was used to evaluate the outbreak response audit. The checklist was based on IDSR 3rd Edition.
Ethical considerations
Written informed consent was obtained from all the respondents. Participants’ names were not included in the study. Confidentiality of all the information collected during the study was maintained. All respondents were interviewed in privacy. Permission to carry out the study was obtained from the Mhondoro-Ngezi District Health Executive (DHE), Mashonaland West Provincial Medical Directorate (PMD) and Health Studies Office.
We interviewed 72 cases and 72 controls. The response rate was 100%. A total of 224 cases were recorded throughout the outbreak. The attack rate was 10 per 1000 population. Males were 69 (95.8%) among the cases and 63 (87.5%) among controls (p=0.07). A total of 36 (50%) cases and 31 (43%) controls (p=0.4) were in the 21-30 years age group. The median age for cases was 28 years (IQR: 23-36), whilst the median age of controls was 30 years (IQR: 25-36). The most common type of employment was artisanal mining, 51 (70.8%) among cases and 64 (88.9%) among controls (p=0.84, Table 1). A total of 55 (76.4%) of the cases and 45 (62.5%) of the controls belonged to the Christian religion (p=0.07). The most reported signs and symptoms in this outbreak were headache, 69 (98.5%) and the least reported was malaise, 46 (65.3%). Most of the cases reported experiencing more than three signs and symptoms.
Case management for calaria cases, Ward 13, Mhondoro-Ngezi District, 2022
A total of 34 (47.2%) were treated at the Battlefields council clinic. Median delay in seeking treatment was 3 days (IQR: 1-5). Thirty-eight (52.8%) were diagnosed during the active case-finding exercise and treated by the mobile health facility. All 72 (100%) cases were treated using Coartemeter and primaquine. Plasmodium falciparum was isolated in all 72 (100%) cases. No severe cases or deaths were reported throughout the outbreak.
Knowledge level on Malaria Among Cases and Controls, Ward 13, Mhondoro-Ngezi District 2022
Overall, a total of 35 (48.6%) of the cases and 36 (50%) of the controls had fair knowledge of malaria (p=0.48). Twenty-two (30.5%) of the cases and 17 (23.6%) of the controls knew malaria complications (p=0.34). Only 22 (30.5) of the cases and 17 (23.6%) of the controls had good knowledge of malaria signs and symptoms (p=0.86). Furthermore, 15 (20.8%) of the cases and 19 (26.4%) of the controls had poor knowledge of malaria (p=0.34).
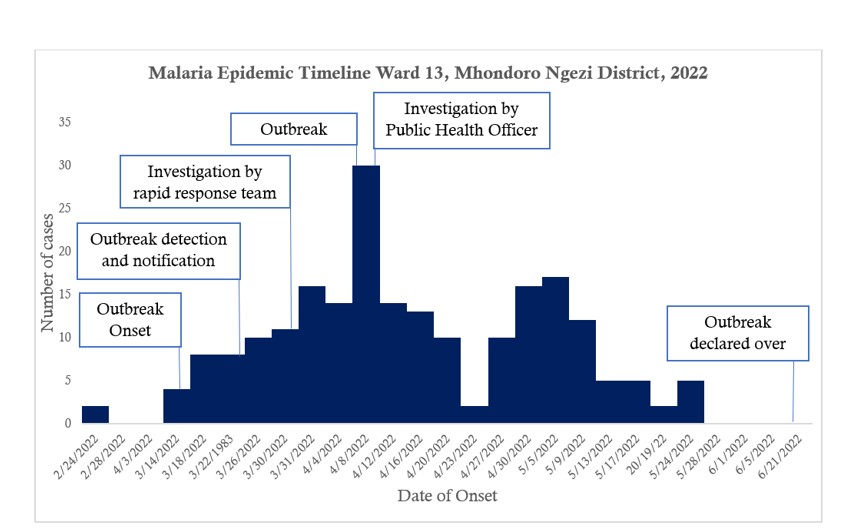
Malaria cases by date of onset, Ward 13, Mhondoro Ngezi district, 2022
Primary cases were recorded on the 24th of February. An increase in the number of malaria cases was recorded at Battlefields council clinic on the 14th of March 2022, signalling the beginning of the outbreak (Figure 1). Most cases occurred within two incubation periods. The outbreak reached its peak on the 9th of April 2022. A decline in cases was experienced from the 3rd to the 25th of May. The Epi-curve suggested a propagated continuous common source where exposure was prolonged. The outbreak was declared over on the 21st of June 2022.
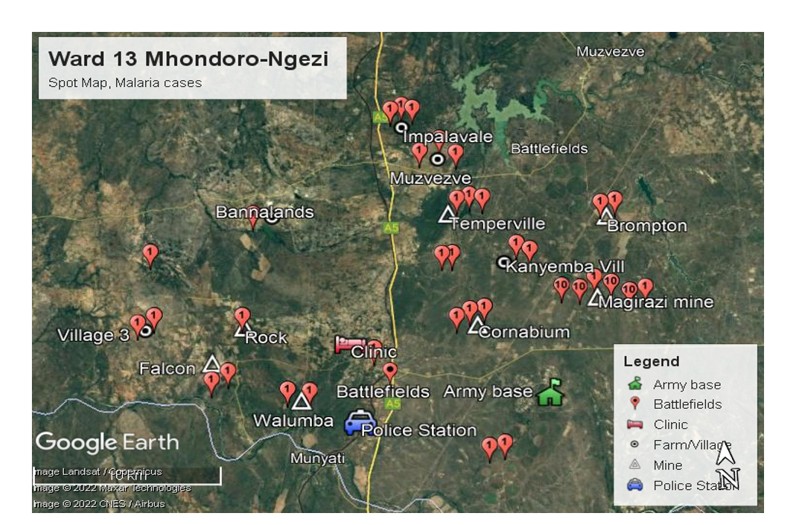
Spatial distribution of malaria cases in Ward 13, Mhondoro-Ngezi 2022 (Figure 2)
The malaria cases are clustered near Magirazi Mine, where 58% of the cases were recorded. Magirazi area is more than 10km away from the Battlefields Council clinic. There were hand-dug pits from mining activities that had accumulated water in the area. The stagnant water sources served as breeding areas for mosquitoes. Brompton area has a flowing river and a dam about 2km away from the residential compound of the mine. The attack rate was 16 per 1,000 population in this area. However, all the other areas that reported cases recorded an attack rate of less than 5 per 1,000 population. Rock mine, Walumba mine and Falcon mine had an attack rate of less than 1 per 1,000.
Factors associated with contracting malaria in Ward 13, Mhondoro-Ngezi District, 2022
Factors that were significantly associated with an increase in malaria transmission in the bivariate analysis were the presence of stagnant water near the sleeping area or home (OR=2.2; 95% CI: 1.03-4.7) and being a permanent resident of ward 13 (OR=7.8; 95% CI: 3.6-17.1) and sleeping outside at night (OR=8.09; 95% CI: 2.06-9.4, Table 2). Significant factors associated with the reduction of transmission of malaria were sleeping in a properly constructed house (OR=0.2; 95% CI: 0.09 – 0.55) and residing outside Ward 13. Sleeping under an insecticide-treated net (ITN) was protective against contracting malaria (OR=0.23; CI: 0.08 – 0.6). Sleeping outside (aOR=4.4; p=0.01), residing permanently in Ward 13 (aOR=7.8; p=0.01), and presence of stagnant water near homes or sleeping areas (aOR=2.2; p=0.01) were independent risk factors associated with contracting malaria in Ward 13, Mhondoro-Ngezi (Table 3).
Environmental assessment
Ward 13, Mhondoro-Ngezi district, is largely a mining area. Almost 75% of the ward is covered by either gold mines or gold claims, and the remaining 25% are communal villages. Illegal mining activities are carried out throughout the ward, including the communal areas. The majority of the people sleep outside in hand-dug pits or in open plastic tents, thereby exposing themselves to mosquito bites. Magirazi area, where most of the cases were clustered, had thick forests with tall grass and vegetation, which act as habitats for mosquitoes. The area received some rainfall prior to and during the course of the outbreak, thereby creating breeding areas. The hand-dug pits became sources of stagnant water, which promoted mosquito breeding. No larval source management was reported prior to the outbreak. Furthermore, plastic containers of opaque beer littered the environment. The plastic container had accumulated water and served as a breeding site for mosquitoes
Entomological investigation, Ward 13, Mhondoro-Ngezi district
Entomological investigations were conducted in Magirazi area, where the majority of the cases were coming from. Larval Source Management (LSM) activities were carried out, and these included scooping and harvesting of mosquito larvae and larviciding of all possible breeding sites. Scooping resulted in the harvesting of approximately 50 mosquito larvae, of which two developed into Anopheles gambiae mosquitoes. No Anopheles mosquitoes were knocked down from pyrethrum spray catches. However, four adult Anopheles mosquitoes were collected from the same area using Prokopak aspirators.
Epidemic preparedness and response audit Ward 13, Mhondoro-Ngezi 2022
A district and facility EPR plan were available but not up to date. However, there were no minutes of EPR committee meetings and the EPR plans were not updated at both the district and facility levels. EPR plan for the district was updated during the first week of January 2022. Nonetheless, there was no evidence of implementation of the plan during the outbreak. The outbreak was detected on the 21 of March 2022 at the health facility and notified to districts on the 29th of March. Battlefields Council Clinic has four nurses and two Environmental health technicians. There was no malaria threshold graph for monitoring cases, thus the delay in identification and notification. Only two nurses were trained in both integrated disease surveillance and response and enhanced malaria case surveillance. There was no spot map of malaria cases displayed at the Battlefields Council clinic. Entomology equipment was available, and funds for outbreak investigation were also availed by the district. No larviciding activities were conducted prior to the outbreak. However, case investigations were being conducted. Malaria cases notified within 24 hours were 47 (65.3%). Entomology investigations were done for 47 (65.3%). Entomology investigations are done for all malaria-positive cases within 7 days. The investigation includes environmental assessments, identification of breeding sites, adult mosquito catches and speciation
Availability of malaria commodities at Battlefields clinic Ward 13, Mhondoro Ngezi district
Battlefields Council Clinic never ran out of malaria medicines throughout the outbreak. Stocks of RDT testing kits and slides for microscopy were adequate and above the 50 and 20 minimum stock, respectively, at the onset of the outbreak. However, shortages of RDTs were experienced during the outbreak in week 16. There was a delay in the supply of RDT test kits from the district stores. Stocks of mosquito nets were also available at the onset of the outbreak. Furthermore, the district had IV fluids required for the management of malaria cases. Oral quinine was available; nevertheless, IV Quinine and SP were out of stock. Slides for microscopy were also available in stock and adequate at the beginning of the outbreak.
The study sought to investigate the factors associated with resurgence of malaria in ward 13, Mhondoro Ngezi district, which is a non-malaria endemic district. The independent risk factors associated with contracting malaria were sleeping outside, sleeping near a stagnant water source and being a permanent resident of Ward 13. The findings were consistent with Masango et. al. (2019)[7], who reported that staying within 3km from a dam or stagnant water sources and staying in poorly constructed houses was associated with malaria transmission. This is biologically plausible since stagnant water sources are known to promote mosquito breeding, leading to the transmission of malaria.
There was a delay in seeking care in most of the cases. Respondents mentioned reluctance to leave their economic activities and distance from the health centre as the major reasons for late treatment seeking. Delay in seeking treatment may have promoted transmission of malaria in ward 13 as the infected persons are a source of mosquitoes’ infection. The findings were similar to Murewanhema et. al. (2017), who reported that a delay in seeking treatment of more than two days increased the chances of transmission of malaria[10]. However, all malaria-positive cases were diagnosed using RDTs. Treatment of all cases was done according to the National malaria case management guidelines for districts in malaria elimination.
There was poor knowledge of signs and symptoms and complications for malaria in both cases and controls. However, overall knowledge level on malaria was fair among both cases and controls. Health education on malaria that was conducted by CHWs prior to the outbreak could have led to overall fair knowledge among cases and controls. However, poor knowledge of signs and symptoms may also explain poor health-seeking behaviour and lack of awareness. Kureya et. al. (2021) also reported that low knowledge of signs and symptoms in a malaria outbreak in Chipinge could have led to poor health-seeking behaviour [11]. The same was also reported by Mundagowa et. al. (2020) in the Beitbridge district of Zimbabwe[12].
Knowledge level between cases and controls was comparable. This could be explained by health education that was offered by PHRRT and VHWs before and during the early days of the outbreak. Cases and controls were comparable except for farmers. The majority of the respondents were males (92%). The ages ranged from 20 to 40 years for both cases and controls. Young individuals, particularly males, are attracted to ward 13 by the prospects in artisanal mining. Similar findings were reported by Mundagowa et. al. (2020), who reported high population of males than females in Beitbridge Ward 6 due to better economic prospects[12].
More cases were recorded in permanent residents of Ward 13 compared with those who resided outside the ward. Individual who stayed outside the ward reported leaving the area before sunset in search of transport and returning early morning on a daily basis. This might have protected them from mosquito bites during the night. Staying close to a stagnant water source was associated with contracting malaria. The ward is associated with manmade pits dug during small scale and illegal mining activities. Accumulation of stagnant water in the pits served as breeding sites for mosquitoes. Sleeping in a properly constructed house reduced the chances of contracting malaria. This was consistent with Masango et. al. (2019)[7] who reported that staying within 3km from a dam or stagnant water sources and staying in poorly constructed houses was associated with malaria transmission. This is biologically plausible since stagnant water sources promote mosquito breeding, leading to the transmission of malaria.
Sleeping outside was associated with contracting malaria. Most cases reported sleeping and working outside during the night, where they would be exposed to mosquito bites. Sleeping under ITNS reduced the risk of contracting malaria. Use of ITNs is known to be protective against mosquito bites and also has a knockdown effect similar to the one provided by chemicals used in indoor residual spraying (IRS). The findings were similar to Murewanhema et. al. (2017), who reported that owning and sleeping under ITNS was protective against malaria transmission[10].
The presence of pits created by artisanal miners that accumulated stagnant water provided breeding opportunities for the Anopheles vector mosquito. Rainfall that was received prior to and during the outbreak resulted in the presence of stagnant water sources that were potential breeding sources for the vector Anopheles mosquito. Plastic containers of opaque beer littered the environment, including the hand-dug pits. The plastic containers had accumulated rainwater. The findings were similar with Amhed et. al. (2021), who reported that the presence of stagnant water increased the chances of contracting malaria[13]. Bayoh et. al. (2011) also reported that larval habitats and populations were concentrated in man-made pits and increased malaria transmission[14]. Community members were not cutting grass and tall vegetation around their households and sleeping areas. Rainfall was also promoting the growth of vegetation in the area. Thick forest and vegetation around sleeping places were providing habitats for the vector mosquitoes, thereby promoting malaria transmission. Muchena et. al. (2017) reported that having long grass around the home was related to the transmission of malaria[3].
Entomological surveillance led to the identification of adult Anopheles mosquitoes. Individuals with a history of travel to malaria areas could also have introduced both the parasite and the vector in the area. Takarinda et. al. (2022) also reported that individuals with a history of travel to Mozambique could have introduced the malaria parasite in Tongogara refugee camp in Manicaland[9].
Detection and notification of the outbreak to the District Medical Officer (DMO) were delayed by seven days. Notification is supposed to be done within 48 hours following detection of the outbreak. Investigation by the rapid response team commenced two weeks into the outbreak. Malaria outbreak investigation should be commenced within 48 hours of notification. Late detection could have been a result of poor surveillance and monitoring of the thresholds by the health facility. This was similar to findings by Takarinda et. al. (2022) who reported that malaria outbreak at Tongogara refugee camp was detected late after 48 hours[9]. Mugwagwa et. al. (2015) also reported poor outbreak detection and response as the reasons for propagated malaria outbreak in Shamva[15].
There was no evidence of the minutes of the EPR meeting. A spot map of cases was not generated. The line list of cases was also not updated. The majority of staff were not trained in outbreak preparedness and response, as well as malaria-enhanced case surveillance. This was similar to findings by Soko et. al. (2015), who reported poor outbreak preparedness and response in Shamva district[16]. The district and health facility were well prepared in terms of medicines and equipment required for malaria case management. However, there was no medicine for the management of complicated cases. This was similar to findings by Manyangadze et. al. (2021), who reported that the health facility was well prepared with all required medicines for malaria case management[17]. Entomology surveillance equipment was available. Resource mobilisation, including transport and fuel, was available throughout the outbreak.
Limitation
The line list was not updated to include suspected and probable cases; therefore, the RDT register was used instead.
Treatment-seeking behaviour was a challenge, as the majority of the cases did not visit the health facility for treatment and were only treated in the community during active case finding. There was, therefore, poor treatment-seeking behaviour among cases. Knowledge was fair among both cases and controls; however, there was poor knowledge of signs and symptoms and complications. Sleeping under an ITNS and sleeping in a properly constructed house were significant protective factors. Significant risk factors were sleeping near a stagnant water source, being a permanent resident of Ward 13 and sleeping outside at night. Identification of adult anopheles mosquitoes may be proof that there is existence of the transmitting vector exists in Ward 13. Outbreak detection and notification standards were not met. EPR team was not meeting quarterly, and there were no minutes of meetings conducted. Health facility workers were not trained in enhanced malaria case-based surveillance. Investigation by the PHRRT was commenced two weeks into the outbreak. We therefore conclude that the district was not well prepared for outbreak response. The following activities were recommended. Health education in the community to be carried out by PHRRT and Battlefields clinic health staff on signs and symptoms, the importance of early treatment seeking behaviour. Distribution of ITNSs and health education on wearing of long-sleeved clothes during night activities and use of mosquito repellents should be done by the EHTs. Filling up and destroying stagnant water sources near sleeping places to be done by community members. Entomological surveillance activities should continue to gather more evidence of the existence of the vector mosquito to inform prevention and control measures. Establishment of vector density and vector mapping should be done. Training of health workers in integrated disease surveillance and response and malaria-enhanced case surveillance should be done.
What is already known about the topic
What this study adds
The study explores factors leading to surges in malaria transmission in areas previously declared free from malaria. Furthermore, the study explores the level of malaria epidemic preparedness in areas deemed to be malaria free.
| Variable | Cases (%) | Controls (%) | p-value |
|---|---|---|---|
| Sex | |||
| Male | 69 (95.8) | 63 (87.5) | 0.07 |
| Female | 3 (4.2) | 9 (12.5) | 0.70 |
| Age (Years) | |||
| ≤10 | 1 (1.4) | 0 (0.0) | 0.31 |
| 11-20 | 6 (8.3) | 5 (6.9) | 0.75 |
| 21-30 | 36 (50.0) | 31 (43.0) | 0.40 |
| 31-40 | 22 (30.6) | 29 (40.3) | 0.22 |
| 41-50 | 6 (8.3) | 4 (5.7) | 0.50 |
| >50 | 1 (1.4) | 3 (4.1) | 0.31 |
| Median age (IQR) | 28(23-36) | 30(25-36) | |
| Level of education | |||
| Secondary | 53 (73.6) | 52 (72.2) | 0.84 |
| Primary | 17 (23.6) | 19 (26.4) | 0.76 |
| Up to grade 6 | 2 (2.8) | 0 (0.0) | 0.15 |
| Never went to school | 0 (0.0) | 1 (1.4) | 0.31 |
| Occupation | |||
| Artisanal miner | 51 (70.8) | 64 (88.9) | 0.84 |
| Farmer | 8 (11.1) | 1 (1.4) | 0.05 |
| Vendor | 6 (8.3) | 2 (2.7) | 0.14 |
| Fisherman | 3 (4.2) | 0 (0.0) | 0.08 |
| *IQR: Interquartile Range | |||
| Variable | Cases n=72(%) | Controls n=72(%) | Odds Ratio | 95% CI | p-value |
|---|---|---|---|---|---|
| Sex: | |||||
| Female | 3 (4.2) | 9 (12.5) | 0.3 | 0.07 — 1.17 | 0.12 |
| Male | 69 (95.8) | 63 (87.5) | |||
| Age (Years): | |||||
| ≥20 | 65 (90.3) | 66 (92.9) | 0.7 | 0.17 — 2.73 | 0.76 |
| <20 | 7 (9.8) | 5 (7.1) | |||
| Occupation: | |||||
| Artisanal miner | 51 (70.8) | 50 (69.4) | 1.06 | 0.51 — 2.18 | 0.85 |
| Other | 21 (26.4) | 22 (30.6) | |||
| History of travel to malarias area | |||||
| Yes | 6 (8.3) | 5 (6.9) | 1.2 | 0.3 — 5.3 | 0.5 |
| No | 66 (9.7) | 67 (93.1) | |||
| Sleeping in properly constructed house | |||||
| Yes | 9 (12.5) | 28 (38.9) | 0.2 | 0.09 — 0.55 | 0.01 |
| No | 63 (87.5) | 44 (61.1) | |||
| Sleeping outside | |||||
| Yes | 57 | 23 | 8.09 | 2.06 — 9.4 | 0.01 |
| No | 15 | 49 | |||
| Stagnant water near sleeping area | |||||
| Yes | 58 (80.6) | 47 (65.3) | 2.2 | 1.03 — 4.7 | 0.03 |
| No | 14 (19.4) | 25 (34.7) | |||
| Permanent resident in Ward 13 | |||||
| Yes | 44 (61.1) | 12 (16.7) | 7.8 | 3.6 — 17.1 | 0.01 |
| No | 28 (38.9) | 60 (83.3) | |||
| Outdoor activities at night | |||||
| Yes | 51 (70.8) | 47 (65.2) | 1.2 | 0.63 — 2.6 | 0.47 |
| No | 21 (29.2) | 25 (34.8) | |||
| Tall grass and vegetation around sleeping area | |||||
| Yes | 64 (88.9) | 67 (93.1) | 1.67 | 0.45-6.84 | 0.28 |
| No | 8 (11.1) | 5 (6.9) | |||
| Owning ITNSs | |||||
| Yes | 6 (8.30 | 25 (34.7) | 0.17 | 0.05 — 0.47 | 0.01 |
| No | 66 (91.7) | 47 (65.3) | |||
| Use of ITNSs | |||||
| Yes | 8 (11.1) | 25 (34.7) | 0.23 | 0.08 — 0.6 | 0.01 |
| No | 64 (88.9) | 47 (63.5) | |||
| ITNSs available at all sleeping places | |||||
| Yes | 7 (9.7) | 26 (36.1) | 0.19 | 0.06 — 0.5 | 0.01 |
| No | 65 (90.3) | 46 (63.9) | |||
| Wearing unprotective clothing | |||||
| Yes | 57 (79.2) | 60 (88.3) | 1.31 | 0.56 — 3.05 | 0.52 |
| No | 15 (20.8) | 12 (16.7) |
| Variable | OR | AOR | 95% CI | p-value |
|---|---|---|---|---|
| Permanent residence in ward 13 | 7.8 | 9.7 | 4 — 23.7 | 0.01 |
| Sleeping outside | 4.4 | 4.7 | 4.7 — 12.4 | 0.01 |
| Stagnant water near sleeping area | 2.2 | 3.7 | 1.4 — 9.6 | 0.01 |