Research | Open Access | Volume 9 (2): Article 89 | Published: 02 Jun 2026

Views: 1,330
Menu, Tables and Figures
| First Author | Year | Country / Region | Income Level | Population / Target Group | Sample Size | Study Design | RCCE Focus | Primary Outcome(s) Measured | Key Findings Summary | Overall Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Dukers-Muijrers, N.H.T.M. | 2023 | Netherlands | High-income | MSM and transgender persons | 1856 | Cross-sectional | Formative | Vaccination willingness | 81.5% willing; higher risk perception, protection motivation, positive norms were enablers; rural residence, lack of community connection were barriers | High |
| Metheny, N. | 2023 | USA | High-income | Marginalized Latino/a/x SGM | Not specified | Cross-sectional | Formative | COVID-19 vaccine uptake; trusted sources | High trust in community organizations and higher education associated with uptake | Moderate |
| Wang, H. | 2022 | Netherlands | High-income | MSM, PrEP users, MSM with HIV | 394 | Cross-sectional | Formative | Perceived concern; perceived risk | MSM with HIV had higher risk perception (aOR 4.29); PrEP users had lower concern | Moderate |
| Vanhamel, J. | 2023 | Belgium | High-income | Mpox cases (primarily MSM) | 139; 12 interviews | Mixed-methods | Formative | Transmission dynamics; self-perceived risk; barriers to detection | Low self-perceived risk and symptom confusion identified as barriers | High |
| Fan, L. | 2024 | Not specified | Not specified | General public online | Not specified | Infodemiology | Infodemiology | Topical/network dynamics; toxicity | High toxicity fuels misinformation; understanding dynamics helps tailor communication | High |
| Jiao, K. | 2023 | China | Upper-middle | YMSM | Large | Cross-sectional | Formative | Mpox risk perception | Large sample; key at-risk population assessed | High |
| Muncaster, K. | 2024 | Not specified | Not specified | At-risk individuals (likely MSM) | Not specified | Mixed-methods | Program evaluation | Access; motivations; stigma | Patient perspectives on access, motivations, and stigma documented | Moderate |
| Ali, Z. | 2024 | Pakistan | Lower-middle | Healthcare workers | Not specified | Cross-sectional | Formative | Mpox vaccine hesitancy | Focus on HCWs in LMIC; hesitancy determinants identified | High |
| da Silva Bulcão, C. | 2024 | Brazil | Upper-middle | General male population | Not specified | Qualitative | Formative | Self-care practices; health beliefs | Rich contextual data on health beliefs and practices | High |
| Wang, Y. | 2024 | USA | High-income | SMMGD individuals on Twitter/X | Not specified | Mixed-methods | Infodemiology | Activism, vaccine, mpox discourse | Innovative BERTopic analysis of online discourse | Moderate |
| Cheung, D.H. | 2024 | Hong Kong, China | High-income | GBMSM | Not specified | Cross-sectional | Formative | Mpox vaccine uptake | Perceptions and information exposure influenced uptake | Moderate |
| Sallam, M. | 2022 | Jordan | Lower-middle | General population | Not specified | Cross-sectional | Formative | Conspiratorial attitudes towards emerging viruses | Conspiratorial attitudes identified as key barrier to RCCE effectiveness | High |
| Sahin, T.K. | 2025 | Turkey | Upper-middle | Cancer patients | 275 | Cross-sectional | Formative | Mpox knowledge; vaccination willingness | 30.9% willing; younger age, prior information, good knowledge were enablers; safety concerns were barriers | Moderate |
| Boutzoukas, A.E. | 2025 | USA | High-income | Sexual minority men | 122 | Cross-sectional | Formative | Barriers to treatment and vaccination; perceived stigma | Stigma (49% believed others would avoid them) and limited vaccine access (30%) documented | Moderate |
| Filardo, T.D. | 2023 | USA | High-income | People experiencing homelessness | 273 | Cross-sectional | Formative | Mpox vaccine acceptability | 59% uptake, 52% willingness; risk perception and vaccine education were enablers; stigma was barrier | High |
| Rajkhowa, P. | 2023 | Global (Twitter data) | Mixed | General public online | 149,133 tweets | Mixed-methods | Infodemiology | Factors influencing vaccination decisions | Identified communication, stigmatization, vaccine accessibility, and safety concerns as key themes | High |
| Paudel, K. | 2023 | Nepal | Lower-middle | MSM | 250 | Cross-sectional | Formative | Mpox knowledge | 87% unaware if contagious; significant knowledge gaps identified | High |
| Rawat, R.S. | 2023 | India | Lower-middle | Medical students/graduates | 404 | Cross-sectional | Formative | Mpox knowledge; sources of knowledge | Only 17.82% had institutional teaching; knowledge gaps documented | Moderate |
| Huang, S. | 2025 | China | Upper-middle | YMSM | 2,079 | Cross-sectional | Formative | Vaccination intention; mpox-related perceptions | Media literacy had positive indirect effect on intentions through perceptions (indirect effect 0.165, p<.001) | High |
| Chen, H.J. | 2024 | China | Upper-middle | MSM | 7,725 | Cross-sectional | Formative | Mpox knowledge awareness rate | 50.1% aware; 79.3% trust official media; new media and social organizations were enablers | High |
| Mahmmoud Fadelallah Eljack, M. | 2023 | Middle East (8 countries) | Mixed | General public | 11,016 | Cross-sectional | Formative | Mpox knowledge; perceptions; predictions | Poor knowledge documented; 61.8% gained awareness from social media | Moderate |
| MohanaSundaram, A. | 2025 | India, Bangladesh | Lower-middle | Health sciences students | 902 | Cross-sectional | Formative | Mpox knowledge; attitudes | Mean knowledge 14.4; 91% relied on vaccination; prior information-seeking via Google/ChatGPT was enabler; misconceptions (55.9% thought antibiotics treat mpox) were barrier | Moderate |
| Youssef, D. | 2023 | Lebanon | Lower-middle | General population | Not specified | Cross-sectional | Formative | Mpox conspiracy beliefs | Social media reliance, poor knowledge, negative attitudes toward government associated with conspiracy beliefs | High |
| Xu, Y. | 2024 | China | Upper-middle | YMSM | 2,493 | Cross-sectional | Formative | Intention to self-isolate; intention to inform close contacts | Higher knowledge (aOR 1.37-1.47), perceived threat, employment were enablers; depression and self-stigma were barriers | Moderate |
| Sallam, M. | 2023 | Jordan | Lower-middle | Healthcare workers | 341 | Cross-sectional | Formative | Mpox vaccination acceptance; vaccine conspiracies | 37.0% accepted; lower conspiracy beliefs and favorable attitude toward mandatory vaccination were enablers | Moderate |
| Nerlich, B. | 2025 | UK | High-income | GBMSM | 91 news items | Qualitative | Formative | Social representations; stigma; identity; coping | Rich qualitative analysis of community narratives; challenging stigma identified as enabler; stigmatizing imagery as barrier | High |
| Chen, C. | 2025 | China (Hubei) | Upper-middle | General population (87.3% MSM) | 63 | Descriptive epidemiology | N/A | Epidemiological characteristics; clinical manifestations | Delayed consultation and unemployment (28.8%) identified as barriers | High |
| Amin, S.M. | 2025 | Egypt | Lower-middle | Nursing students | 505 | Cross-sectional | Formative | Fear, concern, preventive practices | Fear positively predicted practices (B=0.432); lower family income was barrier | High |
| Tendido, M.G. | 2025 | Philippines | Lower-middle | General population | 502 | Cross-sectional | Formative | KAP; predictors of knowledge | Female sex (β=0.130) and higher education (β=0.134) were enablers; low knowledge in certain groups identified | Moderate |
| El Sharif, N. | 2025 | Palestine | Lower-middle | General population | Not specified | Cross-sectional | Formative | Willingness to receive mpox vaccine | 28.8% willing; prior COVID-19 vaccination (aOR 3.07) and trust in vaccines (aOR 6.65) were enablers; misconceptions (33% believe natural immunity sufficient) were barriers | High |
| Gubela, N. | 2026 | Germany (Berlin) | High-income | General population, likely MSM | Not specified | Epidemiological/modelling | Observational | Role of behavior change in outbreak decline | Behavior change contributed significantly to outbreak decline | High |
| Drysdale, K. | 2026 | Not specified | Not specified | LGBTQIA+, people with BBV | Not specified | Qualitative | Formative | Public health and community support needs | Directly relevant to RCCE targeting and community engagement | Moderate |
| Ibrahim, A.M. | 2025 | Not specified | Not specified | Nursing students | Not specified | Quasi-experimental | Intervention evaluation | Effectiveness of health education programme; knowledge improvement | Positive effect on knowledge and attitudes expected | Moderate |
| Bakare, D. | 2024 | Nigeria | Lower-middle | Healthcare workers | Not specified | Cross-sectional | Formative | Mpox knowledge; risk perception | Focus on frontline healthcare workers in Nigeria | High |
| Paterson, A. | 2025 | UK | High-income | General population, at-risk groups | Not specified | Mixed-methods | Formative | Mpox stigma; implications for outbreak control | Directly measures stigma as a key RCCE barrier | Moderate |
| Olawusi, L.F. | 2025 | DRC (Kinshasa) | Low-income | Healthcare workers | Not specified | Cross-sectional | Formative | Determinants of COVID-19 and mpox vaccine hesitancy | Focus on HCWs in low-income, high-risk setting | Moderate |
| Tambo, E. | 2024 | Cameroon | Lower-middle | General population | Not specified | Cross-sectional | Formative | Risk perception; determinants | Directly informs community engagement strategies | High |
| Sahin, T.K. | 2022 | Turkey | Upper-middle | Physicians | Not specified | Cross-sectional | Formative | Mpox knowledge; attitudes towards vaccination | Focus on physicians as key RCCE messengers | High |
| Paradise Vit, A. | 2025 | Not specified | Not specified | Health organizations and public | Not specified | Content analysis | Infodemiology | Topics; emotions; sentiments in posts and responses | Provides insights into health communication on social media | High |
| Boyce, M.R. | 2025 | USA (Chicago) | High-income | Public health department | Not specified | Content analysis | Content analysis | Content and themes of public health communications | Evaluates official RCCE communications on social media | Moderate |
| Cruz Neto, J. | 2024 | Brazil | Upper-middle | Sexual minorities | Not specified | Qualitative | Formative | Stigma; pathologization; social representations | Examines stigma and pathologization in sexual minorities | High |
| Nath, S.D. | 2025 | Bangladesh | Lower-middle | General population | Not specified | Cross-sectional | Formative | Mpox knowledge | Assesses knowledge in general population; knowledge gaps identified | High |
| Olufadewa, I.I. | 2025 | Nigeria | Lower-middle | General population, at-risk groups | Not specified | Qualitative | Formative | Awareness of Mpox; willingness to vaccinate; barriers | Explores barriers to vaccination in community members | Moderate |
| Wu, X. | 2025 | Not specified | Not specified | MSM | Not specified | Quasi-experimental | Intervention evaluation | Mpox knowledge improvement | Directly evaluates RCCE educational intervention for MSM | Moderate |
| Iliyasu, Z. | 2025 | Nigeria (northern) | Lower-middle | PLHIV | Not specified | Cross-sectional | Formative | Risk perception; mpox vaccine acceptability | Focuses on PLHIV as vulnerable population | High |
| Seemanta, S. | 2025 | Not specified | Not specified | Social media users | Not specified | Infodemiology | Infodemiology | Topics; public perception trends over time | Analyzes public perception on Instagram over time | Moderate |
| Al-Fatlawi, N. | 2025 | Iraq | Upper-middle | Healthcare workers and students | Not specified | Cross-sectional | Formative | Knowledge; attitude; anxiety | Assesses KAP and anxiety in healthcare workers and students | Moderate |
| Ito, S. | 2025 | Japan | High-income | Health education content creators | 119 web pages; 30 AI texts | Content analysis | Content analysis | Understandability; actionability; readability | 80% of AI texts scored ≥70%; AI texts more understandable (p<.001); informs material development | High |
| Iliyasu, Z. | 2025 | Nigeria (northern) | Lower-middle | General population | Not specified | Mixed-methods | Formative | Mpox vaccine acceptability; correlates | Mixed methods study on vaccine acceptability | High |
| Ku, K.Y. | 2025 | Not specified | Not specified | Social media users, content creators | Not specified | Content analysis | Infodemiology | Correction approaches; hashtag framing strategies | Examines strategies for countering misinformation on Instagram | High |
| Wang, H. | 2024 | Not specified | Not specified | General population | Not specified | Cross-sectional | Formative | Mpox vaccination willingness | Examines link between information exposure and vaccination willingness | Moderate |
| Zhang, W. | 2024 | China | Upper-middle | Public health stakeholders | Not specified | Qualitative | Formative | Efforts; challenges; recommendations | Provides stakeholder perspectives on mpox prevention and control | High |
| Chan, Z.Y.S. | 2024 | Singapore | High-income | GBMSM | Not specified | Mixed-methods | Formative | Vaccine receptiveness; effective communication strategies | Tailored communication strategies identified as enabler | High |
| Duda, R. | 2024 | Central African Republic | Low-income | General population, at-risk groups | Not specified | Qualitative | Formative | Eco-anthropological and ethnohistorical factors | Provides deep contextual understanding of mpox in CAR | Moderate |
| Wang, Y. | 2024 | USA | High-income | SMMGD individuals | Not specified | Infodemiology | Infodemiology | Topics; discourse patterns; narratives | Analyzes mpox discourse in key population | Moderate |
| Zhang, W. | 2024 | China | Upper-middle | Mpox patients | Not specified | Qualitative | Formative | Patient experiences; implications for prevention | Provides patient perspectives on mpox infection and treatment | High |
| Zheng, M. | 2023 | China | Upper-middle | MSM | Not specified | Observational | Formative | Mpox vaccination hesitancy | National study on vaccine hesitancy in MSM | Moderate |
| Jamil, H. | 2023 | Pakistan | Lower-middle | General population | Not specified | Cross-sectional | Formative | Mpox preventive behaviour | Examines preventive behavior determinants in general population | Moderate |
| Shi, A. | 2023 | Not specified | Not specified | TikTok users | Not specified | Content analysis | Content analysis | Information quality; audience engagement metrics | Analyzes mpox information quality on TikTok | High |
| Ren, F. | 2023 | China (Shenzhen) | Upper-middle | General population | Not specified | Cross-sectional | Formative | Public awareness; specific knowledge; worry | Community-based study on awareness and knowledge; knowledge gaps identified | High |
| Bates, B.R. | 2022 | USA (Ohio) | High-income | Clinicians | Not specified | Cross-sectional | Formative | KAP towards monkeypox | Assesses KAP among clinicians during outbreak | High |
| Reynolds, M.G. | 2013 | Republic of the Congo | Lower-middle | General population | Not specified | Program evaluation | Intervention evaluation | Detection of human monkeypox cases | Intensive community education improved case detection | Moderate |
| Roess, A.A. | 2011 | DRC | Low-income | General population | Not specified | Quasi-experimental | Intervention evaluation | Effectiveness of community intervention | Community intervention improved knowledge, risk perception, and preventive behaviors | High |
| Yellin, H. | 2026 | USA | High-income | SGM, PLHIV | Not specified | Cross-sectional | Formative | Mpox vaccination; willingness to participate in research | Focuses on SGM adults with and without HIV | High |
| Lake, S. | 2025 | Not specified | Not specified | Gay and bisexual men | Not specified | Cross-sectional or qualitative | Formative | Sexual identity-related shame; mpox prevention | Examines shame as barrier to mpox prevention | Moderate |
| Peptan, C. | 2025 | Romania | High-income | General population | Not specified | Longitudinal | Formative | Vaccination acceptance trends; psychosocial perceptions | Analyzes evolution of acceptance over time; anti-vaccination rhetoric identified as barrier | Moderate |
| Jonathan, N.C. | 2025 | Kenya (Kiambu County) | Lower-middle | General population | Not specified | Quasi-experimental | Intervention evaluation | Mpox knowledge | Media campaigns improved knowledge | High |
| WHO | 2022 | WHO European Region | Not applicable | RCCE practitioners | N/A | Guidance | Guidance | Guidance for infodemic management | WHO guidance document on infodemic management | Moderate |
| Biesty, C.P. | 2024 | UK | High-income | GBMSM, community organizations | Not specified | Program evaluation | Intervention evaluation | Stigma reduction; trust increase | Community-led approaches reduced stigma and increased trust | Moderate |
| May, T. | 2023 | UK | High-income | GBMSM | Not specified | Qualitative | Formative | Mpox knowledge; behaviours; barriers | Qualitative study to inform public health messaging | High |
| Kutalek, R. | 2025 | Europe (3 countries) | High-income | RCCE practitioners, civil society | Not specified | Qualitative | Formative | Role of RCCE-IM; reflections; lessons learned | Expert and civil society reflections on RCCE-IM role | High |
| Ikon, A.O. | 2025 | Nigeria (Akwa Ibom) | Lower-middle | General population | Not specified | Program evaluation | Intervention evaluation | Effectiveness of radio jingles | Radio jingles improved health sensitisation | High |
| Maniscalco, D. | 2026 | France (Paris) | High-income | General population, at-risk groups | Not specified | Epidemiological/modelling | Observational | Role of behaviour change in outbreak control | Behaviour change contributed to outbreak control | Moderate |
| Hafeez, U. | 2024 | Pakistan | Lower-middle | General population | Not specified | Cross-sectional | Formative | Knowledge, attitudes, behaviors | Assesses KAB in Pakistani population | High |
| Daroya, E. | 2025 | Canada | High-income | Community, public health actors | Not specified | Qualitative/descriptive | Program description | Collaboration mapping; response description | Describes collaborative model for community-led response | Moderate |
| Novacek, A. | Not specified | Austria | High-income | MSM | Not specified | Cross-sectional | Formative | Mpox vaccine acceptance | Secondary analysis of existing data on vaccine acceptance | Moderate |
| Svartstein, A.W. | 2023 | Denmark | High-income | MSM with HIV | Not specified | Observational | Formative | Mpox incidence; vaccine uptake | Objective data on uptake in high-risk group | High |
| Prochazka, M. | 2024 | Europe, Americas | Mixed | General population, likely MSM | Large | Cross-sectional | Observational | Temporary adaptations to sexual behaviour | Large multi-country study; key behavioural outcome documented | Moderate |
| Boender, T.S. | 2023 | Germany | High-income | Public health institute | N/A | Program description | Program description | Framework establishment; infodemic insights | Describes implementation of core RCCE activity | Moderate |
| Olaoye, A. | 2025 | South Africa | Upper-middle | General population in Eastern Cape | Not specified | Quasi-experimental | Intervention evaluation | Effectiveness for health information promotion | Community radio improved health information | High |
| Xiu, F. | 2024 | Canada | High-income | GBMSM | Not specified | Epidemiological/modelling | Intervention impact evaluation | Impact on mpox transmission | Links past interventions to transmission outcomes | High |
| Pluijmert, D. | 2026 | Aruba | High-income | Community members, stakeholders | Not specified | Qualitative | Formative | Perspectives on risks and prevention | One Health perspective; community views documented | High |
Table 1: Characteristics of included studies on Risk Communication and Community Engagement during mpox outbreaks (n=84).
| First Author | Year | Country / Region | Target Population | Intervention Type | Intervention Description (Brief) | Channel(s) Used | Delivery Mode | Comparator | Primary Outcome(s) | Direction of Effect |
|---|---|---|---|---|---|---|---|---|---|---|
| Reynolds, M.G. | 2013 | Republic of the Congo | General population | Program evaluation | Intensive community education to improve case detection | Community education | Face-to-face | Pre/post | Detection of human mpox cases | Positive |
| Roess, A.A. | 2011 | DRC | General population | Intervention evaluation | Community intervention for mpox prevention | Community engagement | Face-to-face, participatory | Pre/post | Effectiveness for prevention (knowledge, risk perception, preventive behaviors) | Positive |
| Ibrahim, A.M. | 2025 | Not specified | Nursing students | Intervention evaluation | Health education programme on mpox and palliative care | Not specified | Not specified | Pre/post | Knowledge improvement; attitudes toward palliative care | Positive (measured, empirical study findings) |
| Wu, X. | 2025 | Not specified | MSM | Intervention evaluation | Educational intervention to improve mpox knowledge | Not specified | Not specified | Pre/post | Mpox knowledge improvement | Positive (measured, empirical/analytical study findings) |
| Jonathan, N.C. | 2025 | Kenya (Kiambu County) | General population | Intervention evaluation | Impact of social and mainstream media campaigns on knowledge | Social media, mainstream media | Mass media, digital | Exposed vs. unexposed | Mpox knowledge | Positive |
| Olaoye, A. | 2025 | South Africa (Eastern Cape) | General population | Intervention evaluation | Community radio for health information promotion | Community radio | Broadcast | Exposed vs. unexposed | Effectiveness for health information promotion | Positive |
| Ikon, A.O. | 2025 | Nigeria (Akwa Ibom) | General population | Program evaluation | Appraisal of radio jingles for health sensitization | Radio (Passion FM) | Mass media | Exposed vs. unexposed | Effectiveness of radio jingles for health sensitization | Positive |
| Biesty, C.P. | 2024 | UK | GBMSM, community organizations | Program evaluation | Community-led health promotion to counter stigma and increase trust | Community engagement, peer-led | Face-to-face, participatory | Pre/post | Stigma reduction; trust increase | Positive |
Table 2: Characteristics of included RCCE intervention evaluations (n=8)
| Study Design | Assessment Tool Used | High Quality (n, %) | Moderate Quality (n, %) | Low Quality (n, %) | Total (N) |
|---|---|---|---|---|---|
| Quantitative (Cross-sectional) | JBI Checklist for Analytical Cross-Sectional Studies | 30 (57.7%) | 19 (36.5%) | 3 (5.8%) | 52 |
| Qualitative | CASP Qualitative Checklist | 8 (61.5%) | 5 (38.5%) | 0 (0%) | 13 |
| Mixed-Methods | Mixed Methods Appraisal Tool (MMAT) | 4 (57.1%) | 3 (42.9%) | 0 (0%) | 7 |
| Infodemiology / Content Analysis | Adapted WHO/CDC Guidelines; JBI Checklist for Program Evaluation | 3 (60.0%) | 2 (40.0%) | 0 (0%) | 5 |
| Program Evaluation | JBI Checklist for Program Evaluation | 2 (40.0%) | 3 (60.0%) | 0 (0%) | 5 |
| Epidemiological / Modelling | Adapted CASP Checklists | 1 (50.0%) | 1 (50.0%) | 0 (0%) | 2 |
| Total | 48 (57.1%) | 33 (39.3%) | 3 (3.6%) | 84 |
Table 3: Summary of quality appraisal ratings for included studies (n=84) by study design
Augustine Usman Adaka1, Vivian Nwechi1, Maryam Abubakar Umar1, Hannatu Bello1, Polycarp Dauda Madaki2,3,&, Olubunmi Omowumi Olopha1
1Nigeria Centre for Disease Control and Prevention (NCDC), Abuja, Nigeria, 2African Centre of Excellence for Public Health and Toxicological Research (ACE-PUTOR), University of Port Harcourt, PMB 5323, Choba, Port Harcourt, Nigeria, 3Department of Veterinary Tropical Diseases, University of Pretoria, Pretoria, South Africa
&Corresponding author: Polycarp Dauda Madaki, Department of Veterinary Tropical Diseases, University of Pretoria, Pretoria, South Africa, Email: Polycarp.madaki@tuks.co.za ORCID: https://orcid.org/0009-0001-8216-9779
Received: 12 Mar 2026, Accepted: 31 May 2026, Published: 02 Jun 2026
Domain: Infectious Disease Epidemiology
Keywords: Mpox, Risk communication, community engagement, infodemic management, systematic review, health communication, outbreak response, vaccination hesitancy, stigma, misinformation
©Augustine Usman Adaka et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Augustine Usman Adaka et al., Effectiveness of risk communication and community engagement interventions during mpox outbreaks: A systematic review. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):89. https://doi.org/10.37432/jieph-d-26-00080
Introduction: Mpox emerged as a global threat following the 2022 multi-country outbreak. This review evaluates Risk Communication and Community Engagement (RCCE) effectiveness across all affected populations with sustained transmission across diverse populations, with initial concentration among gay, bisexual, and other men who have sex with men (GBMSM). Risk Communication and Community Engagement (RCCE) constitute a fundamental pillar of outbreak response, yet evidence for intervention effectiveness remains fragmented.
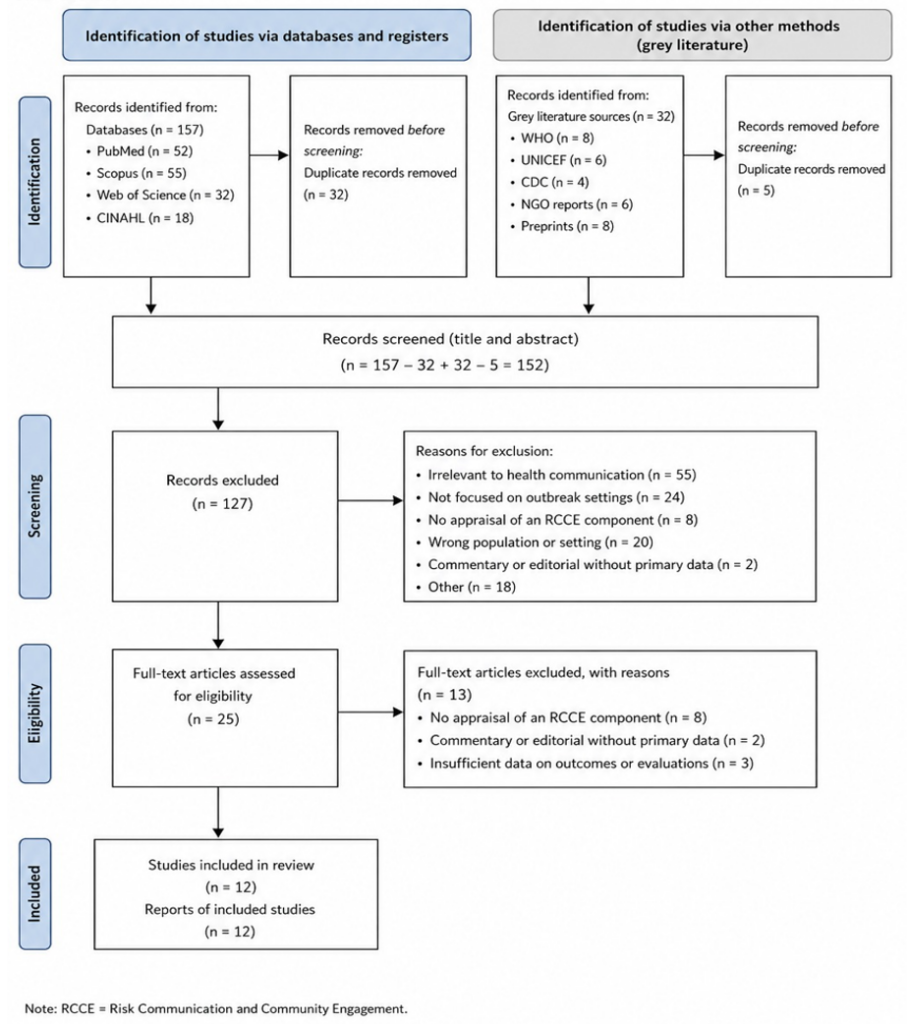
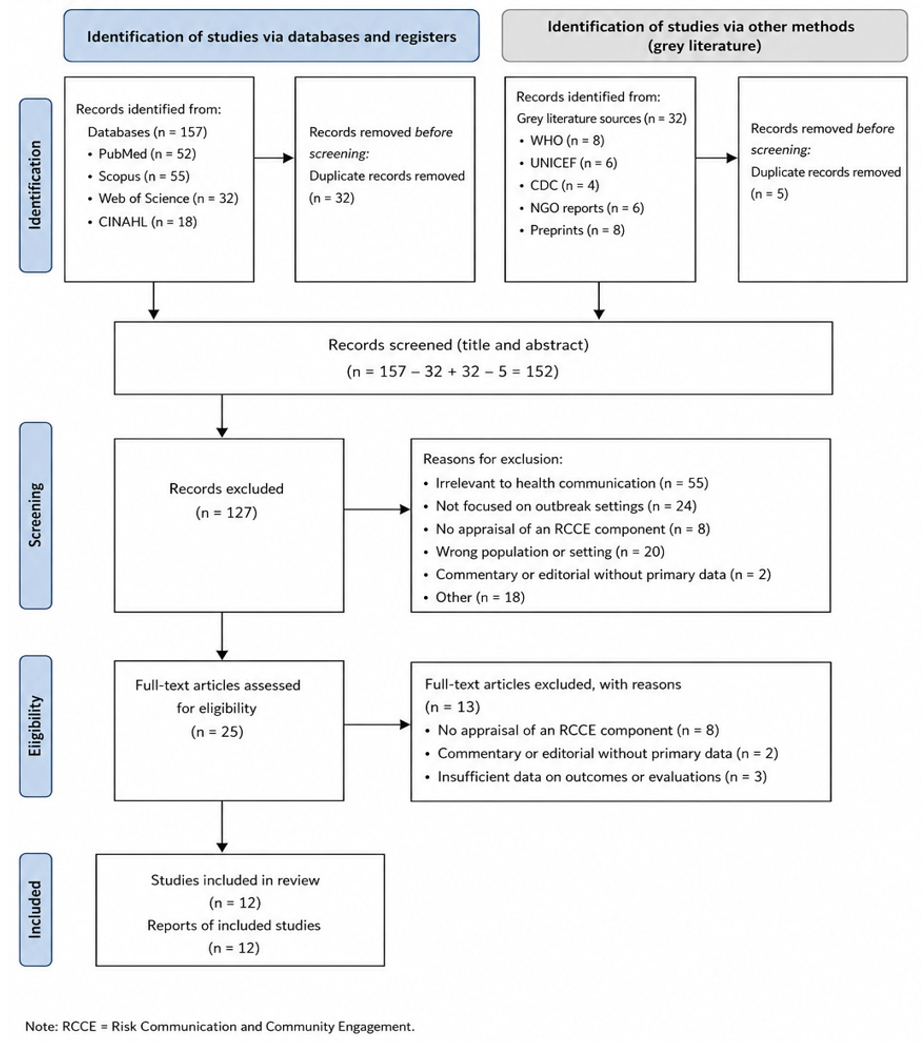
Methods: We conducted a systematic review following PRISMA 2020 guidelines, searching PubMed, Scopus, Web of Science, and Google Scholar. Eligible studies included experimental, observational, mixed-methods, qualitative, and program evaluation designs reporting RCCE interventions or formative research during mpox outbreaks. Two reviewers independently performed screening, data extraction, and quality appraisal.
Results: From 404 records, 84 studies met inclusion criteria. Only eight studies (9.5%) directly evaluated implemented RCCE interventions; 76 (90.5%) were formative research. Studies spanned 35 countries, but 73.8% originated from high- or upper-middle-income countries. Intervention evaluations reported positive effects on knowledge, risk perception, preventive behaviours, case detection, and trust. Formative research documented substantial knowledge gaps (only 50.1% of Chinese MSM demonstrated adequate knowledge), widespread stigma, and vaccination willingness varying from 28.8% in Palestine to 81.5% in the Netherlands. Enablers included tailored communication, trusted messengers, and community participation. Barriers included stigma, conspiracy beliefs, and low risk perception.
Conclusions: While available evidence suggests RCCE interventions can be effective, the evidence base remains thin with a critical imbalance between formative research and rigorous evaluations. Geographical concentration in high-income countries limits generalizability to resource-constrained settings. Future research must prioritise rigorous intervention evaluations to inform evidence-based, equity-oriented RCCE strategies.
Mpox (formerly monkeypox) is a zoonotic disease caused by the mpox virus (MPXV), an Orthopoxvirus comprising two clades: Clade I and Clade II, each with subclades a and b [1]. First identified in humans in 1970, mpox remained endemic in West and Central Africa for decades, with sporadic outbreaks linked to animal-human contact [2]. The global landscape transformed in 2022 when an unprecedented multi-country outbreak of Clade IIb prompted WHO to declare a Public Health Emergency of International Concern (PHEIC) [3]. Unlike prior outbreaks, sustained human-to-human transmission occurred, particularly among sexual networks of gay, bisexual, and other men who have sex with men (GBMSM) [4]. By 2023, African countries experienced a 78.5% surge in suspected cases, and in August 2024, another PHEIC was declared following rapid Clade Ib spread in the Democratic Republic of Congo [4,5]. This evolving transmission landscape demands adaptive public health responses addressing complex social, behavioural, and structural drivers of infection.
Risk Communication and Community Engagement (RCCE), alongside Infodemic Management (IM), constitutes a fundamental pillar of emergency outbreak response [6]. Effective RCCE requires disseminating accurate information and collaborating meaningfully with affected communities to co-create acceptable health guidance [7]. During mpox outbreaks, RCCE has proven essential for reaching marginalized populations, countering stigma, and building trust in vaccination [8]. Interventions encompass community mobilization, mass and social media communication, health education, infodemic management, and community-led health promotion [6]. Effectiveness depends on communication channel appropriateness, messenger credibility, cultural relevance, and genuine community engagement.
Emerging infectious diseases generate infodemics, rapid misinformation spread through digital platforms [9]. During mpox, substantial negative sentiment, homophobia, and misinformation targeted GBMSM communities [10,11]. Effective countermeasures include timely, accessible information, infodemic surveillance, and protection of key populations from misinformation harm [1]. Mpox-related stigma among GBMSM mirrors HIV-era patterns, with anticipated discrimination leading many to delay testing or vaccination [12,13]. Substantial knowledge gaps persist across populations: only 50.1% of Chinese MSM demonstrated adequate knowledge [14]; 87% of Nepalese MSM were unaware whether mpox was contagious [15]. Vaccination willingness varies from 81.5% among Dutch MSM to 28.8% in Palestine [16,17]. Conspiracy beliefs significantly undermine acceptance [18,19]. While GBMSM communities experienced disproportionate initial impact during the 2022 multi-country outbreak, this review adopts a broad, all-population scope to comprehensively evaluate RCCE effectiveness during mpox outbreaks across all affected communities.
While response efforts have reached millions in some settings [20], rigorous evaluations examining RCCE impact on behavioural outcomes and outbreak control remain limited. This systematic review evaluates the effectiveness of RCCE interventions during mpox outbreaks, identifying intervention types, assessing outcomes, examining methodological approaches, and identifying contextual factors that influence effectiveness.
The systematic review was performed and reported following the Preferred Reporting Items of Systematic Reviews and Meta-Analyses (PRISMA) statement (2020) (Page et al., 2021). The review protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) with PROSPERO Registration: CRD420261330594.
Eligibility criteria
The inclusion criteria were predefined and were based on the population, intervention, comparators, outcomes, and study design.
Information sources and search strategy
The development of a comprehensive search strategy was done to identify published and unpublished literature. We searched PubMed, Scopus, Web of Science and Google Scholar databases since their inception up to the search date. The reports and documents of international public health organisations such as the World Health Organization, UNICEF, and the United States Centres for Disease Control and Prevention, websites of government public health agencies, non-governmental organization reports, and preprint archives such as medRxiv and bioRxiv were searched to identify grey literature.
The search strategy was developed iteratively with input from the review team. The strategy combined terms related to three key concepts: mpox, risk communication and community engagement, and evaluation or effectiveness. The complete search strategies for each database are provided in Supplementary File S1. Forward citation tracking of included studies, backward reference searching of all included articles and relevant systematic reviews, and author searches for key researchers in the field were also conducted to identify additional eligible studies.
Study selection
All the records obtained by searches of the database were exported to rayyan systematic review software to remove duplicates and handle the screening. Titles and abstracts were screened by two separate reviewers in reference to the eligibility criteria with the help of a standardised screening form. The disagreements were solved by discussing them, and in cases where an agreement could not be reached, the ultimate decision was made by a third reviewer. Cohen kappa coefficient was used to determine the inter-rater reliability of title and abstract screening.
All potentially eligible studies were then independently retrieved and then assessed by the same two reviewers. Reasons for exclusion at the full-text stage were documented and reported in the PRISMA flow diagram.
Data extraction
A data-extraction form was created using Microsoft Excel and piloted on 5 randomly selected included studies. All the included studies were subject to data extraction by two reviewers, and the differences were resolved via a discussion or consultation with a third reviewer when needed.
The extraction form was used to retrieve bibliometric data, outbreak and contextual data, population data, intervention data, comparators, outcome data and study design data. Other contextual and implementation factors were also elicited, such as the enablers and barriers to the effectiveness of the interventions, equity factors, and the extent of community involvement. In the case of qualitative studies, the essential themes and illustrative quotes pertaining to the RCCE were obtained, and the quantitative and qualitative results were obtained separately in the case of mixed-methods studies.
Quality appraisal and risk of bias assessment
Two reviewers independently evaluated methodological quality and risk of bias using tools suited to each design of the study. The disputes were settled either by consensus or by a third reviewer. Joanna Briggs Institute Checklist was used to evaluate quantitative cross-sectional studies based on the Joanna Briggs Institute Checklist of Analytical Cross-Sectional Studies, and the Critical Appraisal Skills Programme Qualitative Checklist was utilised to evaluate qualitative studies. Mixed-method studies were reviewed by applying the Mixed Methods Appraisal Tool.
Assessment of the infodemiology and content analysis studies was evaluated with modified criteria according to the WHO and CDC guidelines on how to assess surveillance systems with the help of the JBI Checklist on Program Evaluation. Evaluations of program assessments were also done by evaluating the JBI Checklist on Program Evaluation and adaptations of CASP checklists to evaluate epidemiological or modelling studies.
These analyses gave a high, moderate, or low-quality rating to each study based on the analysis. High-quality studies had most or all quality criteria and had limitations that would not significantly influence findings. Moderately rated studies had some methodological limitations, which meant that they could only be cautiously interpreted, and those that had low quality had huge limitations that interfered with confidence in the results. There were no quality exclusion criteria used; nevertheless, quality measures were used to interpret the results during synthesis.
Data synthesis
Given the anticipated heterogeneity in study designs, populations, interventions, and outcome measures, a narrative synthesis was conducted as the primary analytical approach. Studies were organised and summarised using tabulation and thematic grouping based on key characteristics. Relationships between studies were explored by examining patterns in findings across different contexts, populations, and intervention types, and the robustness of the synthesis was assessed by considering the methodological quality of included studies.
Findings were synthesised thematically around the primary and secondary outcomes specified in the review objectives. For each outcome, evidence from intervention studies was synthesised first, followed by evidence from formative research that informed understanding of behavioural and contextual determinants. Qualitative findings were synthesised using thematic synthesis involving line-by-line coding of extracted data, development of descriptive themes, and generation of analytical themes.
Ethical considerations
The review protocol was registered with PROSPERO under registration number CRD420261330594. As this study involved secondary analysis of published and publicly available data, ethical approval was not required. All the studies included were expected to have obtained appropriate ethical approvals as reported in their original publications.
Study selection
PubMed, Scopus, Google Scholar and Web of Science were searched using a systematic search to yield 404 records. The screening of titles and abstracts was done on 292 distinct records after 188 duplicates were eliminated. Two reviewers (AUA and PDM) conducted this screening, and a third reviewer (VN) resolved any differences of opinion. There was high inter-rater reliability (Cohen k = 0.78; 95% CI [0.72, 0.84]), which ensured that there was uniformity in the application of eligibility criteria.
After screening the title and abstract, 194 records were filtered out, and 98 full-text articles were downloaded to undergo further evaluation. Independent screening with full text was performed by the same reviewers and showed an excellent level of agreement (Cohen k = 0.85; 95% CI: 0.78, 0.92). The reasons behind the exclusion at this phase were: (a) no appraisal of an RCCE component (n=8), (b) commentary or editorial in the absence of primary data (n=2), (c) study not about mpox (n=3), and (d) duplicate publication (n=1). Eighty-four studies were finally selected in the qualitative synthesis after passing all inclusion criteria (Figure 1).
NB: The WHO guidance document (WHO, 2022) was included as grey literature informing the background and discussion but was not appraised as an empirical study and is therefore not listed in this table.
Study characteristics, temporal and geographic distribution
Table 1 provides a comprehensive summary of the 84 included studies. The following sections synthesise key characteristics. Publications spanned from 2011 to 2026, with a marked increase following the 2022 multi-country outbreak. Most of the studies (n=76, 90.5%) were conducted during 2022-2026, and this indicates the role that the global health emergency played in driving research activity.
Geographically, the studies were in 35 countries in all six WHO regions. The distribution was:
Income levels, classified by the World Bank, were predominantly high-income (n=40, 47.6%) and upper-middle-income (n=22, 26.2%). Fewer studies originated from lower-middle-income (n=20, 23.8%) and low-income (n=2, 2.4%) settings, highlighting a critical evidence gap in the most resource-constrained contexts.
Study designs and populations
The included studies employed diverse methodological approaches:
Cross-sectional analytical studies (n=52, 61.9%): These formed the backbone of the evidence base, primarily assessing knowledge, attitudes, perceptions, and behavioural intentions.
Target populations reflected the epidemiology of mpox, with gay, bisexual, and other men who have sex with men (MSM) being the most frequently studied group (n=38, 45.2%). Other populations included the general public (n=25, 29.8%), healthcare workers (n=8, 9.5%), and other vulnerable groups such as people living with HIV (PLHIV), cancer patients, people experiencing homelessness, and LGBTQIA+ communities more broadly (n=13, 15.5%).
Categorization of studies: Intervention evaluations vs. formative research
A critical distinction emerged from the data. Only eight studies (9.5%) directly evaluated an implemented RCCE intervention. The remaining 76 studies (90.5%) were classified as formative research, providing essential data on baseline conditions, determinants, and contextual factors necessary for designing effective RCCE strategies. This imbalance underscores the nascent stage of RCCE evaluation science in outbreak contexts. The characteristics of the eight intervention evaluations are summarised in Table 2.
Quality appraisal and risk of bias
Methodological quality was assessed independently by two reviewers (AUA and PDM) using tools appropriate to each study design. Disagreements (n=7) were resolved through consensus with a third reviewer (VN). A summary of quality ratings by study design is presented in Table 3.
Quantitative studies (n=52)
The JBI Checklist for Analytical Cross-Sectional Studies was the primary appraisal tool.
Qualitative studies (n=13)
The CASP Qualitative Checklist was applied.
Mixed-methods studies (n=7)
The Mixed Methods Appraisal Tool (MMAT) was used.
Infodemiology and content analyses (n=5)
Given the absence of a single validated tool, these studies were appraised using adapted criteria from WHO/CDC guidelines for evaluating surveillance systems and the JBI Checklist for Program Evaluation.
Program evaluations (n=5)
Assessed using the JBI Checklist for Program Evaluation.
Epidemiological/modelling studies (n=2)
These were assessed using relevant CASP checklists adapted for modelling studies.
No study was excluded based solely on quality appraisal; however, findings from lower-quality studies were interpreted with greater caution in the narrative synthesis.
Characteristics of RCCE interventions
As detailed in Table 2, the eight intervention evaluations employed diverse strategies, channels, and delivery modes.
Intervention types and channels
The interventions were aimed at direct community engagement. Reynolds et al. (2013) applied face-to-face communication and community meetings as the main aspects of intensive community education applied in the Republic of the Congo. Roess et al. (2011) measured a community-based intervention in the DRC that focused on participatory engagement. Wu et al. (2025) aimed at the educational intervention of MSM, but the channels were not specified. Ibrahim et al. (2025) provided a health education programme to students of nursing in an academic environment.
Duration, implementers, and theoretical foundations
Intervention duration was poorly reported, with most studies (n=6, 75%) not specifying the period over which the intervention was delivered. Implementers varied, including public health authorities, academic institutions, and, crucially, community-based organisations. Only one study (Roess et al., 2011) explicitly mentioned a theoretical framework, and none explicitly incorporated infodemic management or misinformation countering as a core intervention component, although these were mentioned as recommendations in some formative studies.
Synthesis of findings: Effectiveness of RCCE Interventions
Impact on knowledge improvement
Evidence from intervention studies: All four intervention studies measuring knowledge reported positive effects. Wu et al. (2025) found a statistically significant improvement in mpox knowledge among MSM following an educational intervention (effect size not reported). Jonathan et al. (2025) demonstrated that exposure to a multi-media campaign was associated with higher knowledge scores among residents of Kiambu County, Kenya. Olaoye et al. (2025) reported that listeners of Mdantsane FM community radio in South Africa had significantly better health information related to mpox compared to non-listeners. Ikon et al. (2025) similarly found that exposure to radio jingles improved health sensitization on mpox in Akwa Ibom State, Nigeria.
Evidence from formative research: Consistent and often substantial knowledge gaps were documented across diverse populations and settings, reinforcing the critical need for effective knowledge-oriented RCCE. Poor knowledge was documented among:
Impact on risk perception
However, discrepancies in risk perception were also identified. Wang, H. (2022) found that PrEP-using MSM in the Netherlands had lower perceived concern compared to other MSM groups (aOR 2.55 for non-PrEP users having greater concern), suggesting that some sub-populations may underestimate their risk. Vanhamel et al. (2023) identified low self-perceived risk as a barrier to timely healthcare seeking among mpox cases in Belgium.
Impact on preventive behaviours
Barriers to preventive behaviors identified in formative research:
Impact on healthcare-seeking behaviours
Evidence from intervention studies: Reynolds et al. (2013) provided the only direct evidence, showing that intensive community education in the Republic of the Congo led to improved detection of human mpox cases, serving as a proxy for increased healthcare-seeking behavior.
Evidence from formative research: Studies identified significant delays in healthcare seeking. Chen, C. et al. (2025) documented delayed consultation among mpox cases in Hubei Province, China. Vanhamel et al. (2023) found that low self-perceived risk and symptom confusion contributed to these delays. These findings highlight a critical area for future RCCE interventions.
Impact on vaccination uptake and intention
This was the most extensively studied outcome, addressed in 25 studies (29.8%). However, only one intervention study provided direct evidence.
Evidence from intervention studies: Biesty et al. (2024) reported that a community-led health promotion intervention in the UK was effective in increasing trust among priority populations (GBMSM), which is a known precursor to vaccine acceptance. The study did not directly measure changes in vaccination uptake attributable to the intervention.
Evidence from formative research on vaccination intention:
Impact on trust in authorities
Evidence from intervention studies: Biesty et al. (2024) explicitly reported that a community-led approach was effective in increasing trust amongst priority populations. This finding directly supports the value of participatory, community-engaged RCCE.
Evidence from formative research: Trust was identified as both a facilitator and a barrier. High trust in official sources facilitated positive health behaviours (Chen et al., 2024). Conversely, negative attitudes toward the government were associated with higher endorsement of conspiracy beliefs in Lebanon (Youssef et al., 2023), demonstrating that low trust can undermine RCCE efforts.
Impact on misinformation and infodemic management
Evidence from intervention studies: No intervention study explicitly designed to counter misinformation was identified among the included records. However, Ku et al. (2025) analyzed correction approaches on Instagram, finding that specific strategies (e.g., hashtag framing) could be effective in addressing mpox misinformation, offering promising directions for future interventions.
No intervention evaluation explicitly designed to counter misinformation or manage infodemics was identified among the 84 included studies.
Evidence from formative research:
Impact on outbreak metrics
Evidence from intervention studies: Reynolds et al. (2013) used case detection as an outcome measure, demonstrating a link between community education and improved surveillance. Roess et al. (2011) also used surveillance data to assess the impact of their community intervention on mpox prevention.
Evidence from epidemiological studies: Gubela et al. (2026) and Maniscalco et al. (2026) provided the strongest evidence linking population-level behaviours to outbreak control, demonstrating that behaviour change contributed significantly to declining incidence. Xiu et al. (2024) modelled the impact of past interventions on mpox transmission in Canadian cities, suggesting a positive effect.
Healthcare workers as RCCE messengers and recipients
Eight studies focused on healthcare workers (HCWs) as either target populations for RCCE or as potential RCCE messengers. Key findings include: knowledge gaps among HCWs were consistently documented, with only 37.0% of Jordanian HCWs accepting mpox vaccination (Sallam et al., 2023); 17.8% of Indian medical students received institutional mpox teaching (Rawat et al., 2023); and Turkish physicians demonstrated knowledge gaps requiring targeted education (Sahin et al., 2022). In low-income settings, HCW vaccine hesitancy determinants were identified in DRC (Olawusi et al., 2025) and Nigeria (Bakare et al., 2024). The connection between HCW knowledge deficits and their capacity to function as trusted community RCCE messengers was not explicitly examined in any included study. This represents a missed opportunity: HCWs are routinely identified as trusted information sources in outbreak responses, yet no intervention in this review evaluated RCCE strategies designed to improve HCW knowledge specifically to enhance
Eight studies focused on healthcare workers (HCWs) as either target populations for RCCE or as potential RCCE messengers. Key findings include: knowledge gaps among HCWs were consistently documented, with only 37.0% of Jordanian HCWs accepting mpox vaccination (Sallam et al., 2023); 17.8% of Indian medical students received institutional mpox teaching (Rawat et al., 2023); and Turkish physicians demonstrated knowledge gaps requiring targeted education (Sahin et al., 2022). In low-income settings, HCW vaccine hesitancy determinants were identified in DRC (Olawusi et al., 2025) and Nigeria (Bakare et al., 2024). The connection between HCW knowledge deficits and their capacity to function as trusted community RCCE messengers was not explicitly examined in any included study. This represents a missed opportunity: HCWs are routinely identified as trusted information sources in outbreak responses, yet no intervention in this review evaluated RCCE strategies designed to improve HCW knowledge specifically to enhance.
Factors influencing intervention effectiveness: Enablers and barriers
Synthesis of formative and qualitative research, as well as findings from intervention studies, revealed a consistent set of enablers and barriers that influence the effectiveness of RCCE.
Enablers (key success factors)
Barriers (key challenges)
Equity and community participation
Community engagement levels varied across studies. The majority of formative research (n=58, 76.3%) was consultative, using surveys and interviews to inform future strategies. Genuinely participatory or collaborative methods, where communities participated in intervention design decisions, were rare (n=5; Biesty et al., 2024; Daroya et al., 2025; Duda et al., 2024; Kutalek et al., 2025; Nerlich et al., 2025).
To systematically characterize equity dimensions, we applied the PROGRESS-Plus framework (Place of residence, Race/ethnicity/culture/language, Occupation, Gender/sex, Religion, Education, Socioeconomic status, Social capital, Plus other vulnerable groups). Across included studies, reporting of equity-relevant dimensions was inconsistent. Studies explicitly targeting vulnerable or underserved populations included people experiencing homelessness (Filardo et al., 2023), people living with HIV (Iliyasu et al., 2025; Svartstein et al., 2023; Yellin et al., 2026), cancer patients (Sahin et al., 2025), and marginalized sexual and gender minorities (Metheny et al., 2023). However, only two studies (Biesty et al., 2024; Daroya et al., 2025) demonstrated equity-centred intervention design where vulnerable populations were not merely included as subjects but participated in intervention leadership. A critical distinction emerged: inclusion of vulnerable populations in samples (n=12 studies) versus genuine equity-centring in design (n=2 studies). The evidence synthesis reveals a clear gap in low-income countries and in interventions designed and led by affected communities themselves.
Principal findings
This systematic review synthesised 84 studies examining RCCE interventions during mpox outbreaks, revealing a critical imbalance: 90.5% were formative research documenting knowledge, attitudes, and perceptions, while only 9.5% directly evaluated implemented interventions. This disparity reflects the nascent state of RCCE evaluation science in outbreak contexts, consistent with observations from Ebola and COVID-19 reviews, which similarly noted a predominance of descriptive research over intervention effectiveness studies [6,21]. The eight intervention evaluations identified all reported positive effects on primary outcomes, including improved knowledge [22-24], enhanced risk perception [25], increased case detection [26], and reduced stigma with increased trust [27]. However, methodological limitations, weak designs, poor intervention reporting, small sample sizes, and absence of theoretical frameworks limit conclusion strength, mirroring findings from systematic reviews of community engagement in low- and middle-income countries [28]. This evidence base, while promising, remains insufficient to definitively establish which RCCE approaches are most effective across different contexts.
Although GBMSM communities were central to the 2022 outbreak epidemiology, the evidence base for RCCE interventions identified in this review spans general populations, with GBMSM representing one of several priority groups alongside healthcare workers, people experiencing homelessness, and other vulnerable populations.
Geographical and temporal distribution
Research concentrated on high-income (47.6%) and upper-middle-income (26.2%) countries, predominantly in the WHO European Region (33.3%) and the Americas (21.4%). This reflects the 2022 outbreak’s disproportionate initial impact on wealthy nations [3], where rapid transmission among GBMSM networks triggered urgent research responses. However, only 14.3% of studies originated from the AFRO region, with minimal low-income country representation (2.4%), despite Africa bearing the highest historical mpox burden and recent Clade I resurgence [4,5]. This evidence gap raises serious concerns about generalising findings to resource-constrained settings characterised by weaker health systems, lower literacy rates, limited digital access, higher community distrust, and concurrent humanitarian crises [29]. The temporal distribution shows 90.5% of studies published between 2022 and 2026, reflecting the catalytic effect of the PHEIC declaration on research activity. However, the concentration during such a narrow timeframe raises questions about research sustainability as global attention shifts, potentially repeating the pattern of neglect that characterized mpox for decades prior to 2022 [2].
Effectiveness across outcome domains
Knowledge improvement
All four intervention studies measuring knowledge reported positive effects across diverse modalities: targeted MSM education in an unspecified setting [22], multi-media campaigns in Kenya [23], and community radio in South Africa [24]. These findings align with systematic reviews demonstrating that well-designed communication campaigns can significantly improve infectious disease knowledge [30]. However, the substantial knowledge gaps documented across diverse populations in formative research underscore the insufficiency of current RCCE efforts. Only 50.1% of Chinese MSM demonstrated adequate knowledge [14]; 87% of Nepalese MSM were unaware of mpox contagiousness [15]; and healthcare workers showed persistent gaps, with only 17.8% of Indian medical students receiving institutional mpox teaching [31,32]. These gaps are particularly concerning given healthcare workers’ role as trusted community information sources [5] and the direct link between misconceptions and delayed care-seeking [33]. The persistence of knowledge gaps despite widespread information campaigns suggests that passive information dissemination is insufficient and that more intensive, targeted, and culturally tailored approaches are required.
Risk perception
Higher risk perception is consistently associated with greater vaccination willingness [16], stronger self-isolation intentions [34], and increased preventive practices [35], aligning with Health Belief Model constructs [36]. These findings confirm that risk perception operates as a fundamental driver of health-protective behaviours during outbreaks. Critically, risk perception discrepancies were identified: PrEP-using MSM in the Netherlands showed lower concern despite elevated risk [37], illustrating optimistic bias whereby individuals with perceived protection against one infection underestimate risk for others [38]. Low self-perceived risk among Belgian mpox cases contributed to delayed healthcare seeking [33], highlighting a key RCCE target. These findings suggest that effective RCCE must not only provide accurate risk information but actively address cognitive biases leading to risk underestimation, particularly among sub-populations that may feel falsely protected by existing health practices. Messaging should explicitly counter the “not me” phenomenon by personalizing risk and using relatable peer examples.
Preventive behaviours
Epidemiological modelling provided strong evidence for population-level behaviours change, demonstrating that spontaneous sexual behaviours adaptations contributed significantly to outbreak control in Berlin [39] and Paris [40]. A 23-country survey documented widespread temporary behavioural adaptations including reduced partner numbers and avoidance of venues associated with transmission [41], suggesting communities can rapidly modify behaviours when perceiving credible threats. These findings have profound implications: they demonstrate that behaviour change can occur at population level and measurably impact outbreak trajectories, providing strong rationale for investing in behavioural interventions as core outbreak response components. However, identified barriers, stigma [42,43], low risk perception [33], symptom confusion [33], and depression [34], indicate that barrier removal is as important as information provision. RCCE interventions addressing these barriers directly, through stigma reduction, mental health support, and clear symptom recognition guidance, are likely more effective than those focused solely on information provision. The absence of intervention studies measuring behaviour change as a primary outcome represents a missed opportunity to build the evidence base for what works.
Healthcare seeking behaviours
Only one intervention study demonstrated that intensive community education improved case detection in the Republic of Congo [26], serving as a proxy for increased healthcare seeking. Documented delays, up to 9 days in China [44] and Belgium [33], represent substantial transmission windows during which onward transmission can occur. The reasons for delays- low risk perception, symptom confusion, and stigma- are potentially addressable through well-designed RCCE, yet the absence of interventions specifically targeting healthcare seeking constitutes a critical evidence gap. This gap is particularly concerning given that early diagnosis and isolation are fundamental to outbreak control for infectious diseases like mpox [7]. Future RCCE interventions should explicitly target healthcare seeking as a primary outcome, with messages designed to increase symptom recognition, reduce stigma-associated barriers, and provide clear guidance on when and where to seek testing. The success of community education in improving case detection in Congo [26] suggests that similar approaches could be adapted and evaluated in other settings.
Vaccination uptake and intention
Vaccination intention, the most studied outcome (29.8% of studies), showed wide variation: 81.5% among Dutch MSM [16] versus 28.8% in Palestine [17] and 30.9% among Turkish cancer patients [45]. This variation reflects the profound influence of context, population characteristics, and prior health system experiences on vaccine acceptance. Positive determinants, higher risk perception, knowledge, prior vaccination, trust, and positive social norms suggest multi-pathway RCCE approaches addressing multiple determinants simultaneously. Negative determinants, conspiracy beliefs, stigma, rural residence, and safety concerns require active barrier addressing through targeted messaging and community engagement. The association between conspiracy beliefs and lower vaccine acceptance across multiple populations [18,19,46] underscores the critical importance of infodemic management as an integral RCCE component. Trusted messengers consistently mattered: 79.3% of Chinese MSM trusted official media [14]; community organization trust associated with uptake [47]; and knowing vaccinated persons facilitated willingness [16], highlighting the role of social norms and peer influence. These findings suggest that RCCE should invest in partnerships with community-based organizations, train peer messengers, and leverage existing trusted networks rather than relying solely on mass media campaigns.
Trust and misinformation
A community-led UK intervention effectively increased trust among priority populations [27], demonstrating that trust can be built through participatory, community-engaged approaches. High trust facilitated positive behaviours [14]; conversely, negative government attitudes associated with higher conspiracy beliefs in Lebanon [46], demonstrating that low trust can fundamentally undermine RCCE efforts. This finding has relevance for conflict-affected settings where distrust of government and foreign actors is widespread [29]. No intervention explicitly designed to counter misinformation was identified among included studies, despite documented conspiracy belief prevalence [18,19,46] and clear guidance on infodemic management importance [9,11]. This represents a major evidence gap. Ku et al. identified promising Instagram correction strategies [48], suggesting that specific approaches like hashtag framing and corrective messaging could be effective. Infodemic dynamics analyses revealed that high toxicity fuels misinformation [49] and identified key themes, communication, stigmatization, vaccine accessibility, safety concerns—requiring proactive communication [50]. Germany’s infodemic management framework exemplifies institutionalizing social listening and signal detection [51], providing a practical model that should be integrated into all RCCE programmes. The complete absence of IM intervention evaluations represents a critical evidence gap. Despite WHO guidance on infodemic management as a core outbreak response pillar, and despite documented mpox-related misinformation across multiple countries and digital platforms, no study in this review tested an intervention designed to counter misinformation, improve digital health literacy, or reduce the spread of conspiracy beliefs. This gap is particularly concerning given that conspiracy beliefs were significantly associated with lower vaccine acceptance across multiple populations. Future research must prioritize development and rigorous evaluation of IM interventions, including social listening-informed messaging, misinformation correction strategies, and community-led digital health literacy programmes.
Outbreak metrics
Intervention studies linked community education to improved case detection [25,26], demonstrating that RCCE can impact surveillance outcomes. Epidemiological studies demonstrated behaviour change’s contribution to declining incidence [39,40], providing the strongest evidence linking population-level behaviours to outbreak control. These findings validate the fundamental premise of RCCE: that communication and engagement can influence behaviours at sufficient scale to alter epidemic trajectories. Xiu et al. modelled the impact of past interventions on mpox transmission in Canadian cities, suggesting positive effects [52]. However, the small number of studies using outbreak metrics as outcomes limits the evidence base for this critical aspect of RCCE effectiveness. Future evaluations should prioritize objective, population-level outcomes including incidence trends, transmission rates, and vaccination coverage, rather than relying solely on self-reported intentions and attitudes.
Absence of theoretical frameworks in intervention design
Only one of the eight intervention evaluations (Roess et al., 2011) explicitly grounded its approach in a behavioural theory. This absence is not merely a reporting limitation; it has substantive implications for interpreting RCCE effectiveness. Established frameworks such as the Health Belief Model (HBM), the COM-B model (Capability, Opportunity, Motivation – Behaviour), the Theory of Planned Behaviour (TPB), and Social and Behaviour Change Communication (SBCC) frameworks provide structured approaches to identifying behavioural determinants, selecting intervention components, and measuring theoretically specified outcomes. Without explicit theoretical grounding, it is difficult to determine why an intervention worked (or failed), which components were active ingredients, and whether findings can be replicated across different contexts. The seven intervention studies that did not report theoretical frameworks may still have been implicitly theory-informed, but the lack of explicit articulation limits the strength of conclusions that can be drawn and impedes evidence synthesis. Future RCCE intervention research should prospectively apply and report behavioural frameworks to enhance design quality, replicability, and cumulative evidence building.
Enablers and barriers
Synthesis of formative and qualitative research, alongside intervention findings, revealed consistent enablers and barriers influencing RCCE effectiveness. Enablers included: tailored population-specific communication addressing the language, concerns, and contexts of priority populations [16,53]; leveraging trusted messengers including community-based organizations, peer networks, and official media [14,27,47]; community participation and leadership in intervention design and delivery [27,54]; addressing social norms through highlighting peer behaviours [16]; multi-channel approaches combining mass, social, and interpersonal communication [23]; and proactive infodemic management with social listening and rapid response [51]. These enablers align with WHO RCCE guidance principles [7] and findings from community engagement systematic reviews [28,55].
Barriers included: stigma and discrimination discouraging healthcare seeking [42,43] and fueling misinformation [13]; misinformation and conspiracy beliefs eroding trust [18,19,46]; low risk perception leading to low engagement [33,37]; knowledge gaps and misconceptions creating fertile ground for misinformation [14,15,31]; access barriers including limited vaccine access [43], unemployment [44], and rural residence [16]; lack of trust in authorities undermining message acceptance [46]; and inadequate engagement of vulnerable populations including people experiencing homelessness [56] and ethnic minorities [47]. Many barriers are interconnected, stigma fuels misinformation, misinformation erodes trust, low trust reduces engagement, and reduced engagement perpetuates knowledge gaps. Effective RCCE must address this complex web through comprehensive, multi-component interventions rather than isolated information campaigns.
Implications for policy and practice
First, substantial knowledge gaps across diverse populations indicate insufficient current RCCE efforts. National and international RCCE strategies should be reviewed and strengthened, prioritising at-risk populations with accessible, accurate information about mpox transmission, symptoms, and prevention. Second, modifiable determinants of vaccination willingness, risk perception, knowledge, trust, and social norms provide clear intervention targets. Campaigns should address these determinants simultaneously using multi-channel approaches combining mass media with community engagement and peer communication. Third, misinformation prevalence demands integrated infodemic management: investment in social listening systems, rapid response mechanisms for addressing misinformation, and partnerships with social media platforms are urgently needed. Fourth, addressing stigma requires both programmatic responses and legal-policy reforms protecting marginalized populations. RCCE alone cannot eliminate stigma, but can contribute by countering stereotypes, amplifying positive narratives, and engaging affected communities in message development. Fifth, geographical research imbalance calls for investment in research capacity in low- and middle-income countries where mpox has been endemic for decades. International research partnerships that genuinely build local capacity and prioritise locally identified questions should be supported.
Research priorities
Strengths and limitations
Strengths include comprehensive search strategy across multiple databases and grey literature sources; inclusion of diverse study designs enabling synthesis of both effect estimates and contextual insights; dual independent screening, data extraction, and quality appraisal with good inter-rater reliability (κ=0.78-0.85); and PROSPERO registration promoting transparency.
Clade-specific transferability constraints apply. The majority of included studies reflect the 2022 multi-country Clade IIb outbreak, characterized by human-to-human transmission predominantly through sexual networks in urban GBMSM communities. RCCE evidence derived from this context may not generalize straightforwardly to Clade I endemic settings in Central Africa, where transmission dynamics include zoonotic spillover, household and paediatric transmission, and different community perceptions and health-seeking behaviours. Effective RCCE approaches for Clade IIb sexual-network contexts may require fundamental adaptation for Clade I community settings. Future research should evaluate RCCE interventions specifically in Clade I endemic regions.
Limitations: the exclusion of non-English publications potentially introduces language bias. This has specific implications for the African evidence gap: French-language literature from the Democratic Republic of Congo, Cameroon, and other Francophone endemic settings may contain formative or intervention evidence that was not captured, potentially biasing the review towards English-publishing countries and underrepresenting high-burden Francophone Africa. Predominance of cross-sectional studies limiting causal inferences; small number of intervention evaluations precluding meta-analysis; and publication bias, which cannot be excluded. All eight intervention evaluations reported positive effects, and formal statistical assessment (e.g., funnel plot or Egger’s test) was not feasible with only eight studies. Studies with null or negative findings may remain unpublished, which may overestimate the effectiveness of RCCE interventions in this review. Readers should therefore interpret the positive findings with caution. Additional limitations include geographical concentration in high-income countries limiting generalizability to low-resource settings and potential omission of recent publications given the rapidly evolving outbreak landscape. Quality varied across studies, with 57.1% rated high quality, 39.3% moderate, and 3.6% low; findings from lower-quality studies were interpreted with caution.
This systematic review provides comprehensive evidence synthesis on RCCE during mpox outbreaks, revealing both promising findings and critical gaps. While eight intervention studies reported positive effects on knowledge, risk perception, preventive behaviours, and trust, the evidence base remains thin and methodologically weak. Substantial knowledge gaps, misinformation prevalence, stigma impact, and barriers to healthcare seeking and vaccination highlight urgent RCCE strengthening needs. Enablers identified, tailored communication, trusted messengers, community participation, multi-channel approaches, proactive infodemic management, provide a roadmap for more effective interventions. The geographical concentration of research in high-income countries and predominance of formative over evaluative studies underscore the need for sustained investment in RCCE evidence generation, particularly in low-income and conflict-affected settings. Future research must prioritize rigorous intervention evaluations, better reporting, and locally led studies generating contextually relevant evidence. As mpox continues threatening global health security with evolving epidemiology and potential for future outbreaks, the lessons from this review should inform evidence-based, equity-oriented, community-centred RCCE interventions that reach those most in need.
What is already known about the topic
What this study adds
AUA: Conceptualization, Methodology, Supervision, Project administration, writing original draft, Writing – review & editing, Validation. PDM: Conceptualization, Methodology, Formal analysis, Data curation, Visualization, writing original draft, Writing review & editing, Validation. VN, MAU: Investigation, Data curation, Writing review & editing, Validation. HB, OOO: Investigation, Data curation, Visualization, Writing review & editing.
All authors read and approved the final version of the manuscript for publication.
| First Author | Year | Country / Region | Income Level | Population / Target Group | Sample Size | Study Design | RCCE Focus | Primary Outcome(s) Measured | Key Findings Summary | Overall Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Dukers-Muijrers, N.H.T.M. | 2023 | Netherlands | High-income | MSM and transgender persons | 1856 | Cross-sectional | Formative | Vaccination willingness | 81.5% willing; higher risk perception, protection motivation, positive norms were enablers; rural residence, lack of community connection were barriers | High |
| Metheny, N. | 2023 | USA | High-income | Marginalized Latino/a/x SGM | Not specified | Cross-sectional | Formative | COVID-19 vaccine uptake; trusted sources | High trust in community organizations and higher education associated with uptake | Moderate |
| Wang, H. | 2022 | Netherlands | High-income | MSM, PrEP users, MSM with HIV | 394 | Cross-sectional | Formative | Perceived concern; perceived risk | MSM with HIV had higher risk perception (aOR 4.29); PrEP users had lower concern | Moderate |
| Vanhamel, J. | 2023 | Belgium | High-income | Mpox cases (primarily MSM) | 139; 12 interviews | Mixed-methods | Formative | Transmission dynamics; self-perceived risk; barriers to detection | Low self-perceived risk and symptom confusion identified as barriers | High |
| Fan, L. | 2024 | Not specified | Not specified | General public online | Not specified | Infodemiology | Infodemiology | Topical/network dynamics; toxicity | High toxicity fuels misinformation; understanding dynamics helps tailor communication | High |
| Jiao, K. | 2023 | China | Upper-middle | YMSM | Large | Cross-sectional | Formative | Mpox risk perception | Large sample; key at-risk population assessed | High |
| Muncaster, K. | 2024 | Not specified | Not specified | At-risk individuals (likely MSM) | Not specified | Mixed-methods | Program evaluation | Access; motivations; stigma | Patient perspectives on access, motivations, and stigma documented | Moderate |
| Ali, Z. | 2024 | Pakistan | Lower-middle | Healthcare workers | Not specified | Cross-sectional | Formative | Mpox vaccine hesitancy | Focus on HCWs in LMIC; hesitancy determinants identified | High |
| da Silva Bulcão, C. | 2024 | Brazil | Upper-middle | General male population | Not specified | Qualitative | Formative | Self-care practices; health beliefs | Rich contextual data on health beliefs and practices | High |
| Wang, Y. | 2024 | USA | High-income | SMMGD individuals on Twitter/X | Not specified | Mixed-methods | Infodemiology | Activism, vaccine, mpox discourse | Innovative BERTopic analysis of online discourse | Moderate |
| Cheung, D.H. | 2024 | Hong Kong, China | High-income | GBMSM | Not specified | Cross-sectional | Formative | Mpox vaccine uptake | Perceptions and information exposure influenced uptake | Moderate |
| Sallam, M. | 2022 | Jordan | Lower-middle | General population | Not specified | Cross-sectional | Formative | Conspiratorial attitudes towards emerging viruses | Conspiratorial attitudes identified as key barrier to RCCE effectiveness | High |
| Sahin, T.K. | 2025 | Turkey | Upper-middle | Cancer patients | 275 | Cross-sectional | Formative | Mpox knowledge; vaccination willingness | 30.9% willing; younger age, prior information, good knowledge were enablers; safety concerns were barriers | Moderate |
| Boutzoukas, A.E. | 2025 | USA | High-income | Sexual minority men | 122 | Cross-sectional | Formative | Barriers to treatment and vaccination; perceived stigma | Stigma (49% believed others would avoid them) and limited vaccine access (30%) documented | Moderate |
| Filardo, T.D. | 2023 | USA | High-income | People experiencing homelessness | 273 | Cross-sectional | Formative | Mpox vaccine acceptability | 59% uptake, 52% willingness; risk perception and vaccine education were enablers; stigma was barrier | High |
| Rajkhowa, P. | 2023 | Global (Twitter data) | Mixed | General public online | 149,133 tweets | Mixed-methods | Infodemiology | Factors influencing vaccination decisions | Identified communication, stigmatization, vaccine accessibility, and safety concerns as key themes | High |
| Paudel, K. | 2023 | Nepal | Lower-middle | MSM | 250 | Cross-sectional | Formative | Mpox knowledge | 87% unaware if contagious; significant knowledge gaps identified | High |
| Rawat, R.S. | 2023 | India | Lower-middle | Medical students/graduates | 404 | Cross-sectional | Formative | Mpox knowledge; sources of knowledge | Only 17.82% had institutional teaching; knowledge gaps documented | Moderate |
| Huang, S. | 2025 | China | Upper-middle | YMSM | 2,079 | Cross-sectional | Formative | Vaccination intention; mpox-related perceptions | Media literacy had positive indirect effect on intentions through perceptions (indirect effect 0.165, p<.001) | High |
| Chen, H.J. | 2024 | China | Upper-middle | MSM | 7,725 | Cross-sectional | Formative | Mpox knowledge awareness rate | 50.1% aware; 79.3% trust official media; new media and social organizations were enablers | High |
| Mahmmoud Fadelallah Eljack, M. | 2023 | Middle East (8 countries) | Mixed | General public | 11,016 | Cross-sectional | Formative | Mpox knowledge; perceptions; predictions | Poor knowledge documented; 61.8% gained awareness from social media | Moderate |
| MohanaSundaram, A. | 2025 | India, Bangladesh | Lower-middle | Health sciences students | 902 | Cross-sectional | Formative | Mpox knowledge; attitudes | Mean knowledge 14.4; 91% relied on vaccination; prior information-seeking via Google/ChatGPT was enabler; misconceptions (55.9% thought antibiotics treat mpox) were barrier | Moderate |
| Youssef, D. | 2023 | Lebanon | Lower-middle | General population | Not specified | Cross-sectional | Formative | Mpox conspiracy beliefs | Social media reliance, poor knowledge, negative attitudes toward government associated with conspiracy beliefs | High |
| Xu, Y. | 2024 | China | Upper-middle | YMSM | 2,493 | Cross-sectional | Formative | Intention to self-isolate; intention to inform close contacts | Higher knowledge (aOR 1.37-1.47), perceived threat, employment were enablers; depression and self-stigma were barriers | Moderate |
| Sallam, M. | 2023 | Jordan | Lower-middle | Healthcare workers | 341 | Cross-sectional | Formative | Mpox vaccination acceptance; vaccine conspiracies | 37.0% accepted; lower conspiracy beliefs and favorable attitude toward mandatory vaccination were enablers | Moderate |
| Nerlich, B. | 2025 | UK | High-income | GBMSM | 91 news items | Qualitative | Formative | Social representations; stigma; identity; coping | Rich qualitative analysis of community narratives; challenging stigma identified as enabler; stigmatizing imagery as barrier | High |
| Chen, C. | 2025 | China (Hubei) | Upper-middle | General population (87.3% MSM) | 63 | Descriptive epidemiology | N/A | Epidemiological characteristics; clinical manifestations | Delayed consultation and unemployment (28.8%) identified as barriers | High |
| Amin, S.M. | 2025 | Egypt | Lower-middle | Nursing students | 505 | Cross-sectional | Formative | Fear, concern, preventive practices | Fear positively predicted practices (B=0.432); lower family income was barrier | High |
| Tendido, M.G. | 2025 | Philippines | Lower-middle | General population | 502 | Cross-sectional | Formative | KAP; predictors of knowledge | Female sex (β=0.130) and higher education (β=0.134) were enablers; low knowledge in certain groups identified | Moderate |
| El Sharif, N. | 2025 | Palestine | Lower-middle | General population | Not specified | Cross-sectional | Formative | Willingness to receive mpox vaccine | 28.8% willing; prior COVID-19 vaccination (aOR 3.07) and trust in vaccines (aOR 6.65) were enablers; misconceptions (33% believe natural immunity sufficient) were barriers | High |
| Gubela, N. | 2026 | Germany (Berlin) | High-income | General population, likely MSM | Not specified | Epidemiological/modelling | Observational | Role of behavior change in outbreak decline | Behavior change contributed significantly to outbreak decline | High |
| Drysdale, K. | 2026 | Not specified | Not specified | LGBTQIA+, people with BBV | Not specified | Qualitative | Formative | Public health and community support needs | Directly relevant to RCCE targeting and community engagement | Moderate |
| Ibrahim, A.M. | 2025 | Not specified | Not specified | Nursing students | Not specified | Quasi-experimental | Intervention evaluation | Effectiveness of health education programme; knowledge improvement | Positive effect on knowledge and attitudes expected | Moderate |
| Bakare, D. | 2024 | Nigeria | Lower-middle | Healthcare workers | Not specified | Cross-sectional | Formative | Mpox knowledge; risk perception | Focus on frontline healthcare workers in Nigeria | High |
| Paterson, A. | 2025 | UK | High-income | General population, at-risk groups | Not specified | Mixed-methods | Formative | Mpox stigma; implications for outbreak control | Directly measures stigma as a key RCCE barrier | Moderate |
| Olawusi, L.F. | 2025 | DRC (Kinshasa) | Low-income | Healthcare workers | Not specified | Cross-sectional | Formative | Determinants of COVID-19 and mpox vaccine hesitancy | Focus on HCWs in low-income, high-risk setting | Moderate |
| Tambo, E. | 2024 | Cameroon | Lower-middle | General population | Not specified | Cross-sectional | Formative | Risk perception; determinants | Directly informs community engagement strategies | High |
| Sahin, T.K. | 2022 | Turkey | Upper-middle | Physicians | Not specified | Cross-sectional | Formative | Mpox knowledge; attitudes towards vaccination | Focus on physicians as key RCCE messengers | High |
| Paradise Vit, A. | 2025 | Not specified | Not specified | Health organizations and public | Not specified | Content analysis | Infodemiology | Topics; emotions; sentiments in posts and responses | Provides insights into health communication on social media | High |
| Boyce, M.R. | 2025 | USA (Chicago) | High-income | Public health department | Not specified | Content analysis | Content analysis | Content and themes of public health communications | Evaluates official RCCE communications on social media | Moderate |
| Cruz Neto, J. | 2024 | Brazil | Upper-middle | Sexual minorities | Not specified | Qualitative | Formative | Stigma; pathologization; social representations | Examines stigma and pathologization in sexual minorities | High |
| Nath, S.D. | 2025 | Bangladesh | Lower-middle | General population | Not specified | Cross-sectional | Formative | Mpox knowledge | Assesses knowledge in general population; knowledge gaps identified | High |
| Olufadewa, I.I. | 2025 | Nigeria | Lower-middle | General population, at-risk groups | Not specified | Qualitative | Formative | Awareness of Mpox; willingness to vaccinate; barriers | Explores barriers to vaccination in community members | Moderate |
| Wu, X. | 2025 | Not specified | Not specified | MSM | Not specified | Quasi-experimental | Intervention evaluation | Mpox knowledge improvement | Directly evaluates RCCE educational intervention for MSM | Moderate |
| Iliyasu, Z. | 2025 | Nigeria (northern) | Lower-middle | PLHIV | Not specified | Cross-sectional | Formative | Risk perception; mpox vaccine acceptability | Focuses on PLHIV as vulnerable population | High |
| Seemanta, S. | 2025 | Not specified | Not specified | Social media users | Not specified | Infodemiology | Infodemiology | Topics; public perception trends over time | Analyzes public perception on Instagram over time | Moderate |
| Al-Fatlawi, N. | 2025 | Iraq | Upper-middle | Healthcare workers and students | Not specified | Cross-sectional | Formative | Knowledge; attitude; anxiety | Assesses KAP and anxiety in healthcare workers and students | Moderate |
| Ito, S. | 2025 | Japan | High-income | Health education content creators | 119 web pages; 30 AI texts | Content analysis | Content analysis | Understandability; actionability; readability | 80% of AI texts scored ≥70%; AI texts more understandable (p<.001); informs material development | High |
| Iliyasu, Z. | 2025 | Nigeria (northern) | Lower-middle | General population | Not specified | Mixed-methods | Formative | Mpox vaccine acceptability; correlates | Mixed methods study on vaccine acceptability | High |
| Ku, K.Y. | 2025 | Not specified | Not specified | Social media users, content creators | Not specified | Content analysis | Infodemiology | Correction approaches; hashtag framing strategies | Examines strategies for countering misinformation on Instagram | High |
| Wang, H. | 2024 | Not specified | Not specified | General population | Not specified | Cross-sectional | Formative | Mpox vaccination willingness | Examines link between information exposure and vaccination willingness | Moderate |
| Zhang, W. | 2024 | China | Upper-middle | Public health stakeholders | Not specified | Qualitative | Formative | Efforts; challenges; recommendations | Provides stakeholder perspectives on mpox prevention and control | High |
| Chan, Z.Y.S. | 2024 | Singapore | High-income | GBMSM | Not specified | Mixed-methods | Formative | Vaccine receptiveness; effective communication strategies | Tailored communication strategies identified as enabler | High |
| Duda, R. | 2024 | Central African Republic | Low-income | General population, at-risk groups | Not specified | Qualitative | Formative | Eco-anthropological and ethnohistorical factors | Provides deep contextual understanding of mpox in CAR | Moderate |
| Wang, Y. | 2024 | USA | High-income | SMMGD individuals | Not specified | Infodemiology | Infodemiology | Topics; discourse patterns; narratives | Analyzes mpox discourse in key population | Moderate |
| Zhang, W. | 2024 | China | Upper-middle | Mpox patients | Not specified | Qualitative | Formative | Patient experiences; implications for prevention | Provides patient perspectives on mpox infection and treatment | High |
| Zheng, M. | 2023 | China | Upper-middle | MSM | Not specified | Observational | Formative | Mpox vaccination hesitancy | National study on vaccine hesitancy in MSM | Moderate |
| Jamil, H. | 2023 | Pakistan | Lower-middle | General population | Not specified | Cross-sectional | Formative | Mpox preventive behaviour | Examines preventive behavior determinants in general population | Moderate |
| Shi, A. | 2023 | Not specified | Not specified | TikTok users | Not specified | Content analysis | Content analysis | Information quality; audience engagement metrics | Analyzes mpox information quality on TikTok | High |
| Ren, F. | 2023 | China (Shenzhen) | Upper-middle | General population | Not specified | Cross-sectional | Formative | Public awareness; specific knowledge; worry | Community-based study on awareness and knowledge; knowledge gaps identified | High |
| Bates, B.R. | 2022 | USA (Ohio) | High-income | Clinicians | Not specified | Cross-sectional | Formative | KAP towards monkeypox | Assesses KAP among clinicians during outbreak | High |
| Reynolds, M.G. | 2013 | Republic of the Congo | Lower-middle | General population | Not specified | Program evaluation | Intervention evaluation | Detection of human monkeypox cases | Intensive community education improved case detection | Moderate |
| Roess, A.A. | 2011 | DRC | Low-income | General population | Not specified | Quasi-experimental | Intervention evaluation | Effectiveness of community intervention | Community intervention improved knowledge, risk perception, and preventive behaviors | High |
| Yellin, H. | 2026 | USA | High-income | SGM, PLHIV | Not specified | Cross-sectional | Formative | Mpox vaccination; willingness to participate in research | Focuses on SGM adults with and without HIV | High |
| Lake, S. | 2025 | Not specified | Not specified | Gay and bisexual men | Not specified | Cross-sectional or qualitative | Formative | Sexual identity-related shame; mpox prevention | Examines shame as barrier to mpox prevention | Moderate |
| Peptan, C. | 2025 | Romania | High-income | General population | Not specified | Longitudinal | Formative | Vaccination acceptance trends; psychosocial perceptions | Analyzes evolution of acceptance over time; anti-vaccination rhetoric identified as barrier | Moderate |
| Jonathan, N.C. | 2025 | Kenya (Kiambu County) | Lower-middle | General population | Not specified | Quasi-experimental | Intervention evaluation | Mpox knowledge | Media campaigns improved knowledge | High |
| WHO | 2022 | WHO European Region | Not applicable | RCCE practitioners | N/A | Guidance | Guidance | Guidance for infodemic management | WHO guidance document on infodemic management | Moderate |
| Biesty, C.P. | 2024 | UK | High-income | GBMSM, community organizations | Not specified | Program evaluation | Intervention evaluation | Stigma reduction; trust increase | Community-led approaches reduced stigma and increased trust | Moderate |
| May, T. | 2023 | UK | High-income | GBMSM | Not specified | Qualitative | Formative | Mpox knowledge; behaviours; barriers | Qualitative study to inform public health messaging | High |
| Kutalek, R. | 2025 | Europe (3 countries) | High-income | RCCE practitioners, civil society | Not specified | Qualitative | Formative | Role of RCCE-IM; reflections; lessons learned | Expert and civil society reflections on RCCE-IM role | High |
| Ikon, A.O. | 2025 | Nigeria (Akwa Ibom) | Lower-middle | General population | Not specified | Program evaluation | Intervention evaluation | Effectiveness of radio jingles | Radio jingles improved health sensitisation | High |
| Maniscalco, D. | 2026 | France (Paris) | High-income | General population, at-risk groups | Not specified | Epidemiological/modelling | Observational | Role of behaviour change in outbreak control | Behaviour change contributed to outbreak control | Moderate |
| Hafeez, U. | 2024 | Pakistan | Lower-middle | General population | Not specified | Cross-sectional | Formative | Knowledge, attitudes, behaviors | Assesses KAB in Pakistani population | High |
| Daroya, E. | 2025 | Canada | High-income | Community, public health actors | Not specified | Qualitative/descriptive | Program description | Collaboration mapping; response description | Describes collaborative model for community-led response | Moderate |
| Novacek, A. | Not specified | Austria | High-income | MSM | Not specified | Cross-sectional | Formative | Mpox vaccine acceptance | Secondary analysis of existing data on vaccine acceptance | Moderate |
| Svartstein, A.W. | 2023 | Denmark | High-income | MSM with HIV | Not specified | Observational | Formative | Mpox incidence; vaccine uptake | Objective data on uptake in high-risk group | High |
| Prochazka, M. | 2024 | Europe, Americas | Mixed | General population, likely MSM | Large | Cross-sectional | Observational | Temporary adaptations to sexual behaviour | Large multi-country study; key behavioural outcome documented | Moderate |
| Boender, T.S. | 2023 | Germany | High-income | Public health institute | N/A | Program description | Program description | Framework establishment; infodemic insights | Describes implementation of core RCCE activity | Moderate |
| Olaoye, A. | 2025 | South Africa | Upper-middle | General population in Eastern Cape | Not specified | Quasi-experimental | Intervention evaluation | Effectiveness for health information promotion | Community radio improved health information | High |
| Xiu, F. | 2024 | Canada | High-income | GBMSM | Not specified | Epidemiological/modelling | Intervention impact evaluation | Impact on mpox transmission | Links past interventions to transmission outcomes | High |
| Pluijmert, D. | 2026 | Aruba | High-income | Community members, stakeholders | Not specified | Qualitative | Formative | Perspectives on risks and prevention | One Health perspective; community views documented | High |
| First Author | Year | Country / Region | Target Population | Intervention Type | Intervention Description (Brief) | Channel(s) Used | Delivery Mode | Comparator | Primary Outcome(s) | Direction of Effect |
|---|---|---|---|---|---|---|---|---|---|---|
| Reynolds, M.G. | 2013 | Republic of the Congo | General population | Program evaluation | Intensive community education to improve case detection | Community education | Face-to-face | Pre/post | Detection of human mpox cases | Positive |
| Roess, A.A. | 2011 | DRC | General population | Intervention evaluation | Community intervention for mpox prevention | Community engagement | Face-to-face, participatory | Pre/post | Effectiveness for prevention (knowledge, risk perception, preventive behaviors) | Positive |
| Ibrahim, A.M. | 2025 | Not specified | Nursing students | Intervention evaluation | Health education programme on mpox and palliative care | Not specified | Not specified | Pre/post | Knowledge improvement; attitudes toward palliative care | Positive (measured, empirical study findings) |
| Wu, X. | 2025 | Not specified | MSM | Intervention evaluation | Educational intervention to improve mpox knowledge | Not specified | Not specified | Pre/post | Mpox knowledge improvement | Positive (measured, empirical/analytical study findings) |
| Jonathan, N.C. | 2025 | Kenya (Kiambu County) | General population | Intervention evaluation | Impact of social and mainstream media campaigns on knowledge | Social media, mainstream media | Mass media, digital | Exposed vs. unexposed | Mpox knowledge | Positive |
| Olaoye, A. | 2025 | South Africa (Eastern Cape) | General population | Intervention evaluation | Community radio for health information promotion | Community radio | Broadcast | Exposed vs. unexposed | Effectiveness for health information promotion | Positive |
| Ikon, A.O. | 2025 | Nigeria (Akwa Ibom) | General population | Program evaluation | Appraisal of radio jingles for health sensitization | Radio (Passion FM) | Mass media | Exposed vs. unexposed | Effectiveness of radio jingles for health sensitization | Positive |
| Biesty, C.P. | 2024 | UK | GBMSM, community organizations | Program evaluation | Community-led health promotion to counter stigma and increase trust | Community engagement, peer-led | Face-to-face, participatory | Pre/post | Stigma reduction; trust increase | Positive |
| Study Design | Assessment Tool Used | High Quality (n, %) | Moderate Quality (n, %) | Low Quality (n, %) | Total (N) |
|---|---|---|---|---|---|
| Quantitative (Cross-sectional) | JBI Checklist for Analytical Cross-Sectional Studies | 30 (57.7%) | 19 (36.5%) | 3 (5.8%) | 52 |
| Qualitative | CASP Qualitative Checklist | 8 (61.5%) | 5 (38.5%) | 0 (0%) | 13 |
| Mixed-Methods | Mixed Methods Appraisal Tool (MMAT) | 4 (57.1%) | 3 (42.9%) | 0 (0%) | 7 |
| Infodemiology / Content Analysis | Adapted WHO/CDC Guidelines; JBI Checklist for Program Evaluation | 3 (60.0%) | 2 (40.0%) | 0 (0%) | 5 |
| Program Evaluation | JBI Checklist for Program Evaluation | 2 (40.0%) | 3 (60.0%) | 0 (0%) | 5 |
| Epidemiological / Modelling | Adapted CASP Checklists | 1 (50.0%) | 1 (50.0%) | 0 (0%) | 2 |
| Total | 48 (57.1%) | 33 (39.3%) | 3 (3.6%) | 84 |