Research | Open Access | Volume 9 (2): Article 106 | Published: 25 Jun 2026
Views: 21
Menu, Tables and Figures
Table 1: Analysis of Socio-demographic factors associated with Viral Load Suppression Among Adults Living with HIV (N=440)
| Category | Viral Load Suppression | Prevalence Ratio (95% Confidence Interval) | ||
|---|---|---|---|---|
| Suppressed (%) | Unsuppressed (%) | Bivariate analysis | Multivariate analysis | |
| Gender | ||||
| Female | 223 (75.8) | 71 (24.1) | 1.39 (1.27-1.53), p<0.001 | 1.26 (1.14-1.40), p<0.001 |
| Male | 62 (42.5) | 84 (57.5) | Ref. | Ref. |
| Age Group | ||||
| >60 Years | 99 (75.6) | 32 (24.4) | 1.21 (1.09-1.34), p<0.001 | 1.17 (1.06-1.31), p=0.003 |
| 56–60 Years | 78 (66.7) | 39 (33.3) | 1.10 (0.99-1.23), p=0.065 | 1.10 (1.00-1.21), p=0.043 |
| 50–55 Years | 108 (56.3) | 84 (43.7) | Ref. | Ref. |
| Level of Education | ||||
| Primary | 156 (68.4) | 72 (31.6) | 0.92 (0.83-1.03), p=0.174 | 0.95 (0.86-1.05), p=0.393 |
| Secondary | 44 (49.4) | 45 (50.6) | 0.76 (0.67-0.88), p<0.001 | 0.87 (0.76-1.01), p=0.071 |
| Tertiary | 16 (50.0) | 16 (50.0) | 0.77 (0.63-0.93), p=0.009 | 0.84 (0.68-1.03), p=0.101 |
| None | 69 (75.8) | 22 (24.2) | Ref. | Ref. |
| Marital Status | ||||
| Separated/divorced | 59 (69.4) | 26 (30.6) | 1.19 (1.05-1.35), p=0.006 | 1.14 (1.01-1.28), p=0.030 |
| Widow/widower | 150 (72.1) | 58 (27.9) | 1.22 (1.10-1.35), p<0.001 | 1.13 (1.02-1.24), p=0.011 |
| Married/cohabiting | 76 (51.7) | 71 (48.3) | Ref. | Ref. |
| Employment Status | Yes (%) | No (%) | ||
| Employed | 71 (51.1) | 68 (48.9) | 0.81 (0.74-0.90), p<0.001 | 0.88 (0.78-0.99), p=0.037 |
| Unemployed | 214 (71.1) | 87 (28.9) | Ref. | Ref. |
| Livelihood activities | ||||
| Business/trade | 31 (62.0) | 29 (41.4) | 0.89 (0.78-1.02), p=0.103 | 1.02 (0.88-1.18), p=0.741 |
| Formal job/salaried | 23 (60.5) | 14 (50.0) | 0.82 (0.67-1.00), p=0.051 | 1.16 (0.94-1.44), p=0.161 |
| Casual labourer | 62 (42.5) | 19 (38.0) | 0.92 (0.80-1.07), p=0.328 | 1.06 (0.91-1.22), p=0.414 |
| Others | 223 (75.8) | 15 (39.5) | 0.91 (0.77-1.08), p=0.300 | 1.02 (0.88-1.18), p=0.778 |
| Crop cultivation | 14 (50.0) | 78 (30.7) | Ref. | |
| cPR – Crude Prevalence Ratio; aPR – Adjusted Prevalence Ratio; CI: Confidence Interval; Ref: Reference category | ||||
Table 1: Analysis of Socio-demographic factors associated with Viral Load Suppression Among Adults Living with HIV (N=440)
Table 2: Analysis of Dietary practices and physical activity factors associated with viral load suppression among adults on ART (N=440)
| Category | Viral Load Suppression | Prevalence Ratio (95% Confidence Interval) | ||
|---|---|---|---|---|
| Suppressed n (%) | Unsuppressed n (%) | Bivariate analysis (cPR, 95% CI, p) | Multivariate analysis (aPR, 95% CI, p) | |
| Physical Activity | ||||
| Sweeping/gardening/mopping | ||||
| Yes | 194 (63.6) | 111 (36.4) | 0.96 (0.87-1.05), p=0.437 | — |
| No | 91 (67.4) | 44 (32.6) | Ref. | — |
| Walking short or long distances | ||||
| Yes | 91 (61.1) | 58 (38.9) | 0.94 (0.85-1.04), p=0.250 | — |
| No | 194 (66.9) | 97 (33.3) | Ref. | — |
| Riding a motorcycle | ||||
| Yes | 10 (38.5) | 16 (61.5) | 0.75 (0.62-0.91), p=0.004 | 1.03 (0.88-1.18), p=0.696 |
| No | 275 (66.4) | 139 (33.6) | Ref. | Ref. |
| Riding a bicycle | ||||
| No | 255 (89.5) | 120 (32.5) | Ref. | |
| Yes | 30 (10.5) | 35 (49.3) | 0.74 (0.66-0.84), p<0.001 | 0.86 (0.75-0.99), p=0.041 |
| Carrying & transporting harvest | ||||
| Yes | 36 (50.7) | 92 (35.2) | 0.84 (0.74-0.95), p=0.009 | — |
| No | 249 (67.5) | 63 (35.2) | Ref. | — |
| Gardening | ||||
| Yes | 169 (64.8) | 64 (36.6) | 0.99 (0.91-1.09), p=0.991 | — |
| No | 116 (64.8) | 91 (34.3) | Ref. | — |
| Work activities increase heart rate | ||||
| Yes | 111 (63.4) | 64 (36.6) | 0.97 (0.89-1.07), p=0.633 | — |
| No | 174 (65.7) | 91 (34.3) | Ref. | — |
| Intense vigorous activities | ||||
| 4-7 Days | 72 (54.5) | 60 (45.5) | 0.85 (0.75-0.95), p=0.008 | 0.91 (0.81-1.02), p=0.119 |
| 1-3 Days | 125 (68.3) | 58 (31.7) | 0.97 (0.88-1.08), p=0.695 | 1.02 (0.92-1.13), p=0.654 |
| None | 88 (70.4) | 37 (29.6) | Ref. | Ref. |
| Diet | ||||
| Eating Fruits | ||||
| 4-7 Days | 77 (57.5) | 57 (42.5) | 0.80 (0.70-0.91), p=0.001 | 0.96 (0.81-1.14), p=0.677 |
| 1-3 Days | 157 (64.9) | 85 (35.1) | 0.86 (0.76-0.96), p=0.012 | 0.99 (0.85-1.16), p=0.983 |
| None | 51 (79.7) | 13 (20.3) | Ref. | Ref. |
| cPR – Crude Prevalence Ratio; aPR – Adjusted Prevalence Ratio; CI: Confidence Interval; Ref: Reference category | ||||
Table 2: Analysis of Dietary practices and physical activity factors associated with viral load suppression among adults on ART (N=440)
Christine Atuhairwe1,&, Titus Ochieng2
1School of Statistics and Planning, College of Business and Management Sciences, Makerere University, Kampala, Uganda, 2Cabin Uganda Limited
&Corresponding author: Christine Atuhairwe, Makerere University, School of Statistics and Planning, College of Business and Management Studies, Kampala, Uganda, Email: atuhairwek@yahoo.com ORCID: https://orcid.org/0000-0002-8467-2802
Received: 08 Nov 2025, Accepted: 21 Jun 2026, Published: 25 Jun 2026
Domain: Infectious Disease Epidemiology
Keywords: Dietary practices, physical activity, HIV, viral load suppression
©Christine Atuhairwe et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Christine Atuhairwe et al. Dietary practices, physical activity and viral load suppression among adults living with HIV in Uganda. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):106. https://doi.org/10.37432/jieph-d-25-00276
Introduction: Dietary intake and physical activity influence antiretroviral therapy (ART) adherence and health outcomes in people living with HIV. This study assessed their association with viral load suppression (VLS) among adults living with HIV in Uganda.
Methods: A cross-sectional study was conducted from February to August 2024 at 11 The AIDS Support Organization (TASO) Centres of Excellence across Uganda. Data, including viral load results, were collected via questionnaires and medical record abstraction. Descriptive statistics, bivariate, and multivariate from the modified Poisson regression analyses were performed using STATA v18.
Results: Among 440 participants, 64% achieved VLS. Modified Poisson regression revealed that female sex (aPR=1.26, 95%CI: 1.14-1.40, p<0.001), age 56-60 years (aPR=1.10, 95%CI: 1.00-1.21, p=0.043), age >60 years (aPR=1.17, 95%CI: 1.06-1.31, p=0.003), being divorced/separated (aPR=1.14, 95%CI: 1.01-1.28, p=0.030), and widowed (aPR=1.13, 95%CI: 1.02-1.24, p=0.011), were associated with a higher prevalence of VLS. Being employed or active workforce (aPR=0.88, 95% CI: 0.78-0.99, p=0.037), and riding a bicycle (aPR=0.86, 95% CI: 0.75-0.99, p=0.041) were associated with a lower prevalence of VLS in adults.
Conclusion: Viral load suppression among older Ugandan adults on ART was suboptimal. Female sex, older age (56 years and above), and being divorced/separated or widowed were associated with a higher prevalence of viral suppression, whereas being employed/actively working and using a bicycle as a means of transport were associated with a lower prevalence of viral suppression. Targeted interventions are needed to improve treatment outcomes among older adults, particularly among men and those engaged in active employment.
Inadequate food intake substantially impedes antiretroviral therapy (ART) adherence and subsequent viral suppression, particularly in sub-Saharan Africa [1]. Qualitative studies across the region, including Uganda, consistently show a strong association between food scarcity and suboptimal treatment outcomes [1, 2]. Persons living with HIV (PLHIV) frequently interrupt or discontinue ART because treatment-induced hunger is exacerbated when medication is taken on an empty stomach, intensifying side-effects and compromising adherence [1-6]. This fear of hunger and medication-related discomfort often delays ART initiation, thereby reducing the likelihood of achieving sustained viral suppression [1–4].
Although ART can stimulate appetite as a sign of immunologic recovery, it may simultaneously induce gastrointestinal side-effects such as nausea, vomiting, and abdominal pain, which discourage adherence and lead to disengagement from HIV care [2, 4, 6-8]. Qualitative studies in Uganda, Mozambique, and Kenya report that PLHIV experience intensified adverse effects—including headaches, stomach pain, dizziness, chills, tremors, fatigue, fainting, sweating, and rapid heartbeat—especially when taking certain ART regimens without food, significantly impairing daily functioning [2, 4, 6–8].
In many low-resource settings, PLHIV face competing demands to meet essential needs such as food, housing, healthcare, and transportation. These economic pressures may compromise ART adherence behaviours and, in extreme circumstances, force individuals to prioritize immediate survival needs over medication adherence [2, 4–7]. Although these challenges are more frequently documented in resource-limited settings, food-related barriers to adherence have also been reported among socioeconomically disadvantaged PLHIV in higher income countries [9, 10].
It is important to distinguish between food security and dietary practices, as these concepts are related but conceptually distinct and operate through different mechanisms. Food security refers to consistent physical, social, and economic access to sufficient, safe, and nutritious food necessary for an active and healthy life [11, 12]. Food insecurity therefore acts primarily as a structural barrier that limits food availability, stability, and affordability, consequently affecting ART adherence and continuity of care [11, 12].
In contrast, dietary practices refer to actual food consumption behaviours, including meal frequency, dietary diversity, food choices, and the overall quality and combination of foods consumed [13, 14]. Thus, individuals with similar levels of food access may still exhibit markedly different dietary practices. For example, one individual may consume a nutritionally diverse and balanced diet, while another may rely on a monotonous, energy-dense but micronutrient-poor diet. Although food security underpins the ability to maintain healthy eating behaviours, adequate food access alone does not necessarily guarantee optimal dietary quality [13, 14].
This distinction is particularly important in HIV care because interventions targeting dietary practices and patterns address different dimensions of nutrition-related vulnerability. Food security interventions, such as food supplementation, cash transfers, or agricultural support, primarily improve access to food, whereas dietary practice interventions focus on improving dietary quality, diversity, and eating behaviours through nutritional counselling and health education [11, 14]. Both approaches are important for PLHIV but require different indicators and intervention strategies.
Physical activity is increasing recognized as an important component of HIV care particularly among PLHIV, who are at increased risk of metabolic disorders, cardiovascular disease, frailty and functional decline [15, 16]. Behavioural and lifestyle interventions, including physical activity promotion, have been shown to improve ART adherence and overall treatment outcomes among PLHIV [9, 10]. Although the direct effect of physical activity on viral suppression remains incompletely understood, exercise may indirectly improve virologic outcomes through enhanced psychological well-being, reduced depression, improved self-efficacy, and better adherence behaviours [15, 16].
Regular physical activity is being associated with improved mental health, reduced adiposity, enhanced functional status, and better quality of life among PLHIV [15, 16]. However, the relationship between physical activity and HIV outcomes may be complex in low-resource settings, where physically demanding labour may be complex in low-resource settings, where physically demanding labour coexist with inadequate nutritional intake and chronic energy deficits. Among adults living with HIV, excessive physical exertion without adequate nutritional support may contribute to fatigue, undernutrition, and poor treatment outcomes.
Despite growing evidence on the importance of nutrition and physical activity in HIV management, limited research in Uganda in relation to viral load suppression among adults PLHIV. Furthermore, much of the existing literature focuses broadly on food insecurity rather than actual dietary consumption behaviours and dietary patterns. This study therefore explored the relationship between dietary practices—particularly the frequency of fruits, vegetables, and meat consumption as proxy indicators of broader dietary patterns—and physical activity in relation to viral load suppression among adults LHIV in Uganda. The findings may contribute evidence to guide targeted interventions that promote both dietary quality and healthy lifestyle behaviours alongside routine HIV care.
Study Design and Setting
A cross-sectional study was conducted at 11 TASO Centres of Excellences in Uganda: Entebbe, Gulu, Jinja, Masaka, Masindi, Mbale, Mbarara, Mulago, Rukungiri, Soroti, and Tororo. TASO provides comprehensive ART services and supplementary support such as food rations. Pilot testing occurred April–December 2023, with data collection from February–August 2024
Population, sampling and sample size
Adults aged ≥50 years, enrolled in TASO for ≥5 years, and able to communicate in English or a local language were included. A sample size of 440 participants was determined using Yamane’s sample size formula [14], based on an estimated 78% of Uganda’s HIV population on ART [17] and a 5% margin of error. This calculation was adjusted for a potential 10% non-response rate. Participants were selected using systematic random sampling at each TASO site. A medical register of PLHIV, compiled by the clinical officer in charge, served as the sampling frame, with a sampling interval of four employed for selection. Eligibility criteria included: age ≥50 years, confirmed HIV diagnosis, willingness to participate, and ability to communicate in a local language or English. Only those meeting these criteria and providing written informed consent were interviewed at the individual TASO ART Clinics.
Data collection instrument and measurements
A structured questionnaire was used, with questions adapted from lifestyle and behaviour studies that utilized Health Related Quality tools [16]. The primary outcome variable was viral suppression, defined as a viral load of less than 200 copies/mL, consistent with Ministry of Health Uganda guidelines. Viral load results were extracted from the most recent patient medical files (HIV CARD). Viral load was dichotomized into “1” for suppressed (<200 copies/mL) and “0” for unsuppressed (≥200 copies/mL). Viral load testing was performed using GeneXpert, m-Pima, or Abbott Roche machines.
Sociodemographic characteristics, serving as potential explanatory variables, included: sex, age (categorized as 50-55, 56-60, and >60 years), level of education, religious affiliation, marital status, and number of current sexual partners. Other independent variables related to dietary practices and physical activity included: frequency of consumption of fruits, green vegetables, red meat, and white meat. Physical activity was assessed by types of activities (e.g., sweeping, gardening, mopping, riding a bicycle, carrying heavy loads, running, sports) and their frequency (e.g., 1-3 days/week, 4-7 days/week). Employment status, livelihood activities (e.g., crop cultivation, animal rearing, retail trading), and self-reported duration on ART were also captured. Additionally, travel to and from places (using a bicycle or walking) and time spent on these activities, along with recreational activities (e.g., sports, fitness, cultural dances)and alcohol consumption history were included.
Data collection procedures
Sociodemographic variables such as sex, age, level of education, religious affiliations, and marital status were collected. Information on selected protein diets from animal products, fruits, and vegetables, as well as physical activity, was also gathered. The data was collected through face-to-face interviews using the pre-tested questionnaire. The questionnaire was pre-tested using a sample size of 5% from rural and urban areas. Data collection was performed by trained who received intensive training on face-to-face interviews, participant selection, requesting household member participation, administering informed consent, and administering the questionnaire. Completed questionnaires were then entered using EPIDATA and exported to STATA for coding. Further data cleaning and analysis were also conducted using STATA.
Data Analysis
Data were analysed using STATA software (version 18). Descriptive statistics (frequencies, percentages) were used to summarize the characteristics of the study population. Modified Poisson regression models were employed to assess associations between dietary practices, physical activity factors, and viral load suppression. A link test was performed to assess model specification. The predicted value (_hat) was statistically significant (β = 1.36, 95% CI: 0.60–2.10, p < 0.001), while the squared predicted value (_hatsq) was not statistically significant (β = -0.30, 95% CI: -0.89–0.31, p = 0.336). These findings suggest that the model was correctly specified, with no evidence of omitted variables or major specification errors.
Variables with p-values <0.05 in bivariate analysis were considered statistically significant and included in the multivariate analyses. Additionally, age, sex, and marital status were included in the final multivariate model due to their established clinical relevance in HIV viral suppression. Adjusted prevalence ratios (aPR) were reported with their respective 95% confidence intervals (CIs) and p-values. Missing data were handled using complete case analysis.
Ethical Considerations
This study was approved by The AIDS Support Organization (TASO) Institutional Review Board on June 27, 2022 (Ref. No. TASO REC/ADMC010/2022-UG-REC-009), and the Uganda National Council for Science and Technology (UNCST) on January 30, 2023 (Ref.No. SS1396ES). In accordance with the principles outlined in the Declaration of Helsinki, all participants were fully informed about the study’s objectives, potential risks, and benefits. Participants were reassured that their confidentiality would be maintained and that their participation was entirely voluntary. Prior to the interviews, written informed consent was obtained from each participant, ensuring their understanding of the study’s purpose and willingness to participate.
Participants sociodemographics characteristics
A total of 440 eligible participants were interviewed across TASO’s Centres of Excellence (COEs) in Entebbe, Gulu, Jinja, Masaka, Masindi, Mbale, Mbarara, Mulago, Rukungiri, Soroti, and Tororo. The cohort’s mean age was 58.3 ± 6.8 years, with a median age of 57 years (interquartile range: 53–62 years). Forty-three per cent (43%) of participants were between 50 and 55 years old. Demographically, 66.0% of the participants were female, and 46.0% reported being widowed. Regarding educational attainment, 52.0% had completed primary level education.
Bivariate analysis showed that female participants had a significantly higher likelihood of achieving viral load suppression relative to males (cPR=1.39, 95% CI: 1.27–1.53, p<0.001). Participants aged above 60 years had a significantly higher likelihood of achieving VLS compared with those aged 50–55 years (cPR=1.21, 95% CI: 1.09–1.34, p<0.001). The association for those aged 56–60 years was marginally non-significant (cPR=1.10, 95% CI: 0.99–1.23, p=0.065). Participants with Secondary education (cPR=0.76, 95% CI: 0.67–0.88, p<0.001) and tertiary education (cPR=0.77, 95% CI: 0.63–0.93, p=0.009) were less likely to achieve viral load suppression compared to those with no formal education. Separated/divorced (cPR=1.19, 95% CI: 1.05–1.35, p=0.006) and widowed participants (cPR=1.22, 95% CI: 1.10–1.35, p<0.001) were significantly more likely to achieve VLS than those who were married or cohabiting. Employed participants had a significantly lower likelihood of VLS than unemployed participants (cPR=0.81, 95% CI: 0.74–0.90, p<0.001). None of the livelihood activity categories showed statistically significant associations with VLS, although formal employment approached significance (cPR=0.82, 95% CI: 0.67–1.00, p=0.051).
After adjustment for potential confounders, female sex remained significantly associated with a higher prevalence of VLS (aPR=1.26, 95% CI: 1.14–1.40, p<0.001). Older age groups also showed significant associations, with participants aged 56–60 years (aPR = 1.10, 95% CI: 1.00–1.21, p = 0.043) and those above 60 years (aPR = 1.17, 95% CI: 1.06–1.31, p = 0.003) more likely to achieve suppression compared with those aged 50–55 years. Marital status remained influential, as separated/divorced (aPR = 1.14, 95% CI: 1.01–1.28, p = 0.030) and widowed participants (aPR = 1.13, 95% CI: 1.02–1.24, p = 0.011) had a higher prevalence of suppression relative to married/cohabiting participants. Employment status was also significant, with employed participants having a lower prevalence of suppression (aPR = 0.88, 95% CI: 0.78–0.99, p = 0.037). No independent associations were observed for education level or livelihood activity categories (Table 1).
Dietary practices and physical activity of older adults living with HIV
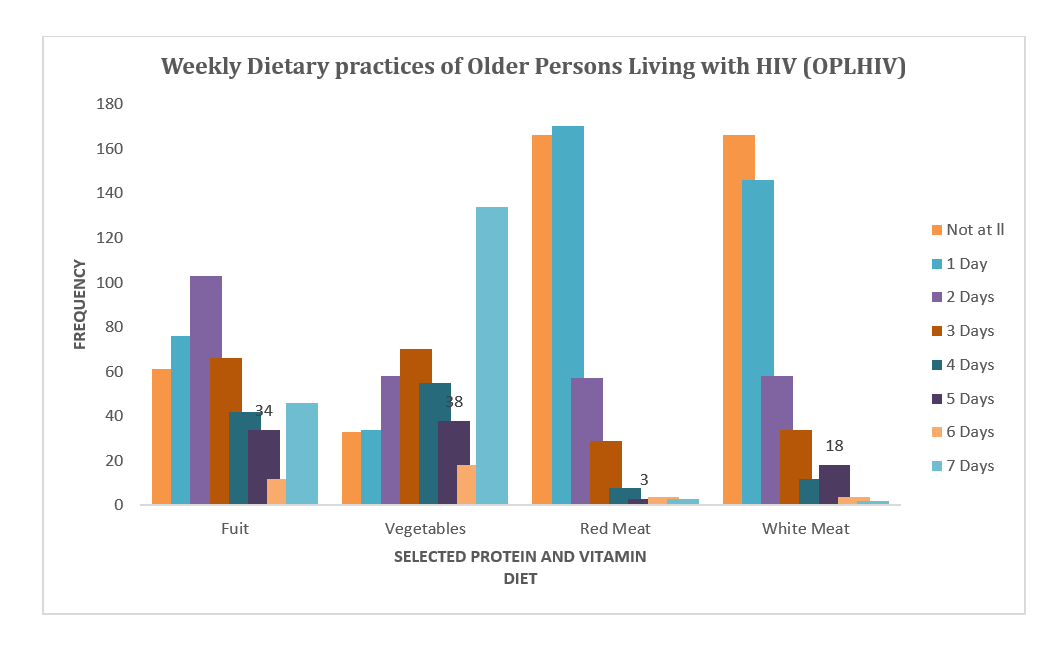
Among participants, distinct dietary patterns were observed. White meat consumption was reported by 33% once a week, while 36% consumed red meat weekly. A substantial portion (30%) consumed vegetables daily, and approximately 23% ate fruits twice weekly. When asked about overall weekly intake, 56% reported eating fruit 1–3 days a week, and 56% consumed vegetables 4–7 days a week. More than half (60%) ate red meat, and 62% ate white meat at least once weekly (Figure 1).
Unemployment was prevalent, affecting 68% of the participants, with 58% of those unemployed engaged in crop cultivation. Physical activity levels varied. Only 30% of participants engaged in intense vigorous physical activity (e.g., walking >2 mph, shovelling, carrying heavy loads, digging large plots) in a typical week. However, 39% reported work that elevated their heart rate, and approximately 70% participated in light activities like sweeping, yard work, and gardening. Other common physical activities included walking (34%), bicycling (17%), transporting farm harvests (e.g., bananas, cassava, potatoes) (16%), and gardening/digging (59%). Regarding travel, 36% of older adults LHIV walked or cycled 4-7 days a week, with 32% spending at least 60 minutes on such travel. Only 23% of PLHIV reported that their antiretroviral therapy (ART) medications affected their movements. Participation in recreational activities (e.g., sports, fitness, cultural dances) was reported by 23% of respondents, with 26% engaging at least once weekly.
At the bivariate level, several physical activity and dietary factors were significantly associated with viral load suppression. Participants who reported riding a motorcycle had a 25% lower likelihood of achieving viral load suppression compared with non‑riders (cPR = 0.75, 95% CI: 0.62–0.91, p = 0.004). Similarly, bicycle riding was associated with a 26% lower likelihood of suppression (cPR = 0.74, 95% CI: 0.66–0.84, p < 0.001), while carrying and transporting harvest was associated with a 16% lower likelihood (cPR = 0.84, 95% CI: 0.74–0.95, p = 0.009). In addition, participants engaging in vigorous physical activity for 4–7 days per week were less likely to achieve viral load suppression compared with those reporting no vigorous activity (cPR = 0.85, 95% CI: 0.75–0.95, p = 0.008).
Dietary factors also demonstrated significant associations with viral load suppression. Compared with participants who did not consume fruits, those consuming fruits for 1–3 days per week (cPR = 0.86, 95% CI: 0.76–0.96, p = 0.012) and 4–7 days per week (cPR = 0.80, 95% CI: 0.70–0.91, p = 0.001) had a lower likelihood of achieving suppression. Similar patterns were observed for vegetable intake, where consumption for 1–3 days per week (cPR = 0.83, 95% CI: 0.72–0.96, p = 0.012) and 4–7 days per week (cPR = 0.79, 95% CI: 0.69–0.91, p = 0.001) was associated with reduced likelihood of suppression. Weekly consumption of red meat (cPR = 0.83, 95% CI: 0.76–0.91, p < 0.001) and white meat (cPR = 0.83, 95% CI: 0.76–0.91, p < 0.001) was likewise associated with lower prevalence of suppression. Participation in sports, fitness, and recreational activities was linked to an 11% lower likelihood of suppression (cPR = 0.89, 95% CI: 0.79–0.99, p = 0.037). Other physical activity, transportation, alcohol use, and smoking variables showed no statistically significant associations with viral load suppression.
After controlling for potential confounders, most of the associations observed at the bivariate level were attenuated and no longer statistically significant. Riding a bicycle remained the only factor independently associated with viral load suppression, with bicycle riders having a 14% lower likelihood of achieving suppression compared with non‑riders (aPR = 0.86, 95% CI: 0.75–0.99, p = 0.041). In contrast, the associations between viral load suppression and motorcycle riding, vigorous physical activity, fruit and vegetable consumption, red and white meat intake, participation in sports and recreational activities, exercise frequency, alcohol use, and transportation‑related activities were no longer statistically significant after adjustment. (Table 2).
This study investigated dietary practices, physical activity, and their association with viral load suppression in adults living with HIV. The observed viral suppression rate of 64% remains substantially below the UNAIDS 95-95-95 targets, emphasising persistent gaps in HIV care among the ageing population. To improve outcomes, the existing HIV care models must combine ART management with geriatric and non-communicable disease services within regional TASO centres. Such an approach may address the multiple health challenges faced by people ageing with HIV, including comorbidities, functional limitations, and socioeconomic barriers that may affect treatment outcomes [17, 18]. Similar variability in viral suppression has been documented across sub-Saharan African countries, where differences in retention in care, adherence support, socioeconomic conditions and health system capacity contribute to varying treatment outcomes [23, 27].
The significantly higher prevalence of viral suppression among older women compared to men suggest important gender-related disparities in HIV treatment outcomes. Older women were more likely to achieve viral suppression than their male counterparts. This finding is consistent with studies from sub-Saharan Africa showing that women generally exhibit better ART adherence, healthcare utilization, and retention in care than men [18, 19]. Similar findings have been reported in Rwanda where male gender was associated with unsuppressed viral loads [18], although findings from other settings, such as Zambia, have been less consistent [20]. The higher suppression rates observed in women in this study are likely attributable to their more consistent treatment adherence, proactive care-seeking behaviours, and potentially healthier lifestyle choices, including lower alcohol consumption, typically observed compared to men [18, 18, 20]. The observed gender disparity highlights the need for male-friendly HIV care interventions that improve treatment adherence and engagement in care among older men.
Additionally, older age was associated with better viral suppression. Participants aged 56 years and older were significantly more likely to achieve VLS compared with those aged 50–55 years. This finding may reflect greater treatment experience, longer ART exposure, more stable lifestyles and stronger coping mechanisms among older individuals. Older participants who remain engaged in HIV care over prolonged periods may also develop routines that support medication adherence and clinic attendance. Previous studies have reported mixed findings regarding the relationship between age and viral suppression. While some studies in sub-Saharan Africa have found that older adults are more likely to achieve viral suppression, others indicate that younger age predicts virologic failure and rebound [18-21]. Nevertheless, the current findings support evidence suggesting that older adults may achieve better treatment outcomes because of accumulated treatment experience and greater stability in health-seeking behaviours.
Separated/divorced and widowed participants were more likely to achieve viral suppression compared to married or cohabiting participants. These findings reflect differences in household responsibilities, caregiving obligations, healthcare autonomy, or flexibility in attending clinic visits. Married individuals may experience competing family demands, disclosure concerns, or other psychosocial challenges that affect consistent ART use and clinic attendance. Although limited evidence exists regarding marital status and viral suppression among older adults living with HIV, these findings suggest that household and relationship contexts may play an important role in treatment outcomes and should be considered when designing adherence support interventions.
Employment was positively associated with a lower likelihood of viral suppression. Employed or older adults still in active employment were less likely to achieve viral suppression compared with unemployed participants. This finding may reflect competing work-related demands, time constraints, mobility requirements, or difficulties attending clinic appointments and maintaining optimal adherence schedules. In many low-resource settings, employment among older adults often involves labour-intensive activities, informal work arrangements, and long working hours that may interfere with consistent engagement in HIV care [18-20]. Similar observations have been reported in settings where occupational commitments limit healthcare utilization and adherence to treatment schedules. These findings highlight the importance of flexible and differentiated HIV service delivery models that accommodate the needs of working older adults. An important finding of this study was that riding a bicycle remained independently associated with a lower likelihood of viral suppression after adjustment for potential confounders. Older adults who reported riding a bicycle were less likely to achieve viral suppression compared with non-riders. This finding may reflect underlying socioeconomic and occupational circumstances rather than a direct adverse effect of cycling itself. In rural Ugandan settings, bicycle use is often common among individuals engaged in physically demanding livelihoods and may serve as a proxy for lower socioeconomic status, longer travel distances, food insecurity, or increased daily physical demands. These factors may reduce opportunities for optimal adherence, clinic attendance, and overall engagement in HIV care. Similar observations have been reported in resource-limited settings where physically demanding lifestyles and economic vulnerability contribute to poorer HIV treatment outcomes.
Several physical activity variables, including motorcycle riding, carrying and transporting harvests, participation in vigorous activities, and recreational sports, were associated with viral suppression in the bivariate analysis. However, these associations were no longer statistically significant after adjustment for other factors. This suggests that the observed relationships were likely explained by underlying sociodemographic characteristics, economic factors, or other confounding influences rather than independent effects of physical activity.
While physical activity remains important for maintaining cardiovascular health, physical functioning, and quality of life among older adults living with HIV, the present findings do not provide evidence that most physical activity indicators independently influence viral suppression. This study showed a negative association between vigorous physical activity (4-7 days/week), heavy farm labour and viral suppression. While moderate physical activity is generally beneficial for cardiovascular and metabolic health, excessive physical exertion among people living with HIV may produce adverse physiological consequences when not accompanied by adequate nutritional intake [15, 16]. In resource-limited settings, intense manual labour may create a state of chronic negative energy balance characterized by insufficient caloric and protein replacement relative to energy expenditure [12]. Among PLHIV, this may accelerate protein-energy malnutrition, sarcopenia, and micronutrient depletion. These conditions can impair immune recovery, reduce ART tolerance, and exacerbate chronic inflammation.
This finding directly contradicts with literature demonstrating positive effects of moderate physical activity on health outcomes in people living with HIV [15, 16]. Emerging HIV nutrition literature further suggests that chronic under nutrition weakens gut mucosal integrity and promotes microbial translocation, where bacterial products enter systemic circulation and sustain immune activation despite ART use [1, 13]. Excessive physical labour in nutritionally vulnerable populations may intensify these inflammatory pathways and compromise virologic control. Similar observations have been reported in studies among ageing with HIV in low-income settings, where physically demanding livelihoods combined with inadequate food supplies contribute to poorer treatment outcomes and nutritional frailty.
Similarly, fruit consumption, vegetable consumption, and intake of red and white meat were significantly associated with viral suppression in the bivariate analysis but lost statistical significance in the multivariable model. The disappearance of these associations after adjustment suggests that individual food groups were not independently associated with viral suppression in this study population. These findings indicate that the relationship between nutrition and virologic outcomes may be more complex than can be captured through assessment of individual food items alone. Contemporary nutritional epidemiology recognizes that foods consumed in combination, their synergistic interactions among nutrients, food diversity, meal composition and dietary quality collectively influence immune function, inflammatory pathways, metabolic health, and gut microbiota composition [13, 14]. The absence of independent associations between specific food groups and viral suppression should not be interpreted as evidence that nutrition is unimportant in HIV management. Rather, it may reflect limitations of food-frequency measures, which do not adequately capture portion sizes, dietary diversity, meal composition, food preparation methods, overall dietary quality, or long-term nutritional adequacy. Contemporary nutritional epidemiology recognizes that foods are consumed in combination and that synergistic interactions among nutrients collectively influence immune function, inflammation, metabolic health, and gut microbiota composition [13, 14]. Dietary patterns, therefore, provide a more comprehensive representation of nutritional exposure than analyses based on individual foods.
Several studies among PLHIV have demonstrated that greater dietary diversity scores are associated with improved ART adherence, enhanced immune recovery, better nutritional status, and reduced systemic inflammation [1, 13]. Diverse dietary patterns rich in fruits, legumes, vegetables, whole grains and lean proteins provide synergistic combinations of micronutrients, antioxidants, essential fatty acids, and dietary fibre that collectively support immune regulation and intestinal integrity [1, 13]. Nutrients such as zinc, selenium, omega-3 fatty acids, vitamins A, C, D and E and plant-derived antioxidants work synergistically to reduce oxidative stress, improve mucosal immunity and support CD4+T-cell recovery [1, 13].
Emerging evidence further suggests that dietary patterns influence the gut microbiome and intestinal barrier function, both of which are critical in HIV disease progression and immune recovery [13]. Studies among PLHIV have shown that low-diversity diets characterized by refined carbohydrates and limited micronutrient intake are associated with dysbiosis, microbial translocation, and persistent immune activation despite ART use [13-15]. In contrast, diversified dietary patterns containing fibre-rich plant foods, fermented foods, and omega-3-rich protein sources have been linked to improved gut microbial diversity and reduced inflammatory markers [18, 19]. This relationship is particularly relevant among the ageing, where chronic inflammation and immunosenescence already contribute to accelerated physiological decline.
The lack of association between individual food frequencies and viral suppression in this study may also reflect limitations inherent in food-frequency-based assessments, which do not adequately capture overall dietary quality or nutritional adequacy. An individual may frequently consume fruits or vegetables yet remain nutritionally vulnerable if total caloric intake, protein intake, or dietary diversity is insufficient.
Consequently, future nutritional research among older adults living with HIV should move beyond isolated food-frequency measures and employ more comprehensive approaches such as dietary diversity scores, repeated 24-hour dietary recalls, and dietary pattern analyses. Longitudinal studies incorporating anthropometric indicators, inflammatory biomarkers, micronutrient assessments, and measures of gut health would further enhance understanding of the biological pathways linking nutrition, physical activity, and viral suppression in ageing populations living with HIV. Conversely, monotonous diets commonly observed in low-resource settings may provide sufficient caloric satiety while remaining deficient in micronutrient density and dietary diversity. Diets predominantly composed of maize meal, cassava, or matooke with infrequent intake of protein-rich and micronutrient-dense foods may fail to meet the complex nutritional demands of ageing individuals living with HIV [1, 13, 15]. Such dietary patterns may contribute to persistent inflammation, reduced immune resilience, nutritional frailty, and impaired physiological recovery despite adequate ART adherence.
These findings suggest that HIV nutritional interventions should move beyond simplistic single-food recommendations towards the promotion of diverse, balanced, and contextually appropriate dietary patterns. Nutritional counselling for adults with HIV should therefore emphasize dietary diversity, adequate caloric intake, balanced macronutrient consumption, and inclusion of locally available anti-inflammatory foods such as leafy vegetables, legumes, silverfish (mukene), fermented foods, and other micronutrient-rich traditional foods [13-15].
Overall, the findings suggest that viral suppression among older adults living with HIV is influenced more strongly by sociodemographic and socioeconomic factors than by individual dietary practices or physical activity behaviours. Interventions aimed at improving treatment outcomes should prioritize male engagement in care, support for working older adults, and strategies that address broader social and economic barriers to adherence while continuing to promote healthy lifestyles and adequate nutrition as essential components of comprehensive HIV care.
Limitations
This study has several limitations. First, it captured only selected dietary practices (specific food groups) and therefore did not assess their direct influence on viral load suppression. Second, self-reported data on dietary practices and physical activity are subject to recall bias and social desirability bias. Finally, the study was conducted among older participants attending TASO centres, which may not be fully representative of all adults with HIV in Uganda, particularly those who are not enrolled in care or attend other facilities.
The viral load suppression rate remains suboptimal, highlighting a critical gap in achieving global HIV targets. Female gender, older age (over 60 years), and certain marital statuses (separated, divorced, or widowed) were associated with higher odds of viral suppression. Contrary to expectations, engaging in intense vigorous physical activity and employment showed negative associations with viral suppression, suggesting complex interactions between livelihood, physical exertion, and health outcomes in this vulnerable population. These findings underscore the need for targeted public health interventions for ageing with HIV in Uganda, particularly focusing on improving viral suppression among men, younger older adults, married individuals, and those engaged in physically demanding livelihoods. Future research should explore the underlying mechanisms linking intense physical activity to suboptimal viral suppression and investigate additional factors such as the quality and quantity of food intake, economic stability beyond employment status, and access to comprehensive care services.
What is already known about the topic
What this study adds
By collecting data from 11 TASO Centres of Excellence across major regions of Uganda, the study provides valuable real- world evidence from one of the country’s leading HIV care provider. This broad geographical reach enhances the generalizability and practical relevance of the findings within the Ugandan context, particularly in routine HIV care settings.
The findings identify associations between various dietary and physical activity patterns and viral suppression among those ageing with HIV. These findings provide important evidence for the development of tailored, evidence based lifestyle interventions that can be integrated into existing HIV care programs to improve health outcomes for the ageing HIV population.
Unlike studies that assess only general dietary or activity levels, this study examined specific dietary components including frequency of fruits, green vegetables, red meat, and white meat consumption, as well as the types/frequencies of physical activities as sweeping, gardening, mopping, cycling, carrying heavy loads, running, sports. This detailed approach offers more actionable insights for designing culturally and contextually appropriate interventions for those ageing with HIV.
The authors extend their deepest gratitude to the older infected persons who participated in the study without whom this research wouldn’t have been possible. We thank the staff of TASO facilities in Entebbe, Gulu, Jinja, Masaka, Masindi, Mbale, Mbarara, Mulago, Rukungiri, Soroti and Tororo where the study was conducted.
Table 1: Analysis of Socio-demographic factors associated with Viral Load Suppression Among Adults Living with HIV (N=440)
| Category | Viral Load Suppression | Prevalence Ratio (95% Confidence Interval) | ||
|---|---|---|---|---|
| Suppressed (%) | Unsuppressed (%) | Bivariate analysis | Multivariate analysis | |
| Gender | ||||
| Female | 223 (75.8) | 71 (24.1) | 1.39 (1.27-1.53), p<0.001 | 1.26 (1.14-1.40), p<0.001 |
| Male | 62 (42.5) | 84 (57.5) | Ref. | Ref. |
| Age Group | ||||
| >60 Years | 99 (75.6) | 32 (24.4) | 1.21 (1.09-1.34), p<0.001 | 1.17 (1.06-1.31), p=0.003 |
| 56–60 Years | 78 (66.7) | 39 (33.3) | 1.10 (0.99-1.23), p=0.065 | 1.10 (1.00-1.21), p=0.043 |
| 50–55 Years | 108 (56.3) | 84 (43.7) | Ref. | Ref. |
| Level of Education | ||||
| Primary | 156 (68.4) | 72 (31.6) | 0.92 (0.83-1.03), p=0.174 | 0.95 (0.86-1.05), p=0.393 |
| Secondary | 44 (49.4) | 45 (50.6) | 0.76 (0.67-0.88), p<0.001 | 0.87 (0.76-1.01), p=0.071 |
| Tertiary | 16 (50.0) | 16 (50.0) | 0.77 (0.63-0.93), p=0.009 | 0.84 (0.68-1.03), p=0.101 |
| None | 69 (75.8) | 22 (24.2) | Ref. | Ref. |
| Marital Status | ||||
| Separated/divorced | 59 (69.4) | 26 (30.6) | 1.19 (1.05-1.35), p=0.006 | 1.14 (1.01-1.28), p=0.030 |
| Widow/widower | 150 (72.1) | 58 (27.9) | 1.22 (1.10-1.35), p<0.001 | 1.13 (1.02-1.24), p=0.011 |
| Married/cohabiting | 76 (51.7) | 71 (48.3) | Ref. | Ref. |
| Employment Status | Yes (%) | No (%) | ||
| Employed | 71 (51.1) | 68 (48.9) | 0.81 (0.74-0.90), p<0.001 | 0.88 (0.78-0.99), p=0.037 |
| Unemployed | 214 (71.1) | 87 (28.9) | Ref. | Ref. |
| Livelihood activities | ||||
| Business/trade | 31 (62.0) | 29 (41.4) | 0.89 (0.78-1.02), p=0.103 | 1.02 (0.88-1.18), p=0.741 |
| Formal job/salaried | 23 (60.5) | 14 (50.0) | 0.82 (0.67-1.00), p=0.051 | 1.16 (0.94-1.44), p=0.161 |
| Casual labourer | 62 (42.5) | 19 (38.0) | 0.92 (0.80-1.07), p=0.328 | 1.06 (0.91-1.22), p=0.414 |
| Others | 223 (75.8) | 15 (39.5) | 0.91 (0.77-1.08), p=0.300 | 1.02 (0.88-1.18), p=0.778 |
| Crop cultivation | 14 (50.0) | 78 (30.7) | Ref. | |
| cPR – Crude Prevalence Ratio; aPR – Adjusted Prevalence Ratio; CI: Confidence Interval; Ref: Reference category | ||||
Table 2: Analysis of Dietary practices and physical activity factors associated with viral load suppression among adults on ART (N=440)
| Category | Viral Load Suppression | Prevalence Ratio (95% Confidence Interval) | ||
|---|---|---|---|---|
| Suppressed n (%) | Unsuppressed n (%) | Bivariate analysis (cPR, 95% CI, p) | Multivariate analysis (aPR, 95% CI, p) | |
| Physical Activity | ||||
| Sweeping/gardening/mopping | ||||
| Yes | 194 (63.6) | 111 (36.4) | 0.96 (0.87-1.05), p=0.437 | — |
| No | 91 (67.4) | 44 (32.6) | Ref. | — |
| Walking short or long distances | ||||
| Yes | 91 (61.1) | 58 (38.9) | 0.94 (0.85-1.04), p=0.250 | — |
| No | 194 (66.9) | 97 (33.3) | Ref. | — |
| Riding a motorcycle | ||||
| Yes | 10 (38.5) | 16 (61.5) | 0.75 (0.62-0.91), p=0.004 | 1.03 (0.88-1.18), p=0.696 |
| No | 275 (66.4) | 139 (33.6) | Ref. | Ref. |
| Riding a bicycle | ||||
| No | 255 (89.5) | 120 (32.5) | Ref. | |
| Yes | 30 (10.5) | 35 (49.3) | 0.74 (0.66-0.84), p<0.001 | 0.86 (0.75-0.99), p=0.041 |
| Carrying & transporting harvest | ||||
| Yes | 36 (50.7) | 92 (35.2) | 0.84 (0.74-0.95), p=0.009 | — |
| No | 249 (67.5) | 63 (35.2) | Ref. | — |
| Gardening | ||||
| Yes | 169 (64.8) | 64 (36.6) | 0.99 (0.91-1.09), p=0.991 | — |
| No | 116 (64.8) | 91 (34.3) | Ref. | — |
| Work activities increase heart rate | ||||
| Yes | 111 (63.4) | 64 (36.6) | 0.97 (0.89-1.07), p=0.633 | — |
| No | 174 (65.7) | 91 (34.3) | Ref. | — |
| Intense vigorous activities | ||||
| 4-7 Days | 72 (54.5) | 60 (45.5) | 0.85 (0.75-0.95), p=0.008 | 0.91 (0.81-1.02), p=0.119 |
| 1-3 Days | 125 (68.3) | 58 (31.7) | 0.97 (0.88-1.08), p=0.695 | 1.02 (0.92-1.13), p=0.654 |
| None | 88 (70.4) | 37 (29.6) | Ref. | Ref. |
| Diet | ||||
| Eating Fruits | ||||
| 4-7 Days | 77 (57.5) | 57 (42.5) | 0.80 (0.70-0.91), p=0.001 | 0.96 (0.81-1.14), p=0.677 |
| 1-3 Days | 157 (64.9) | 85 (35.1) | 0.86 (0.76-0.96), p=0.012 | 0.99 (0.85-1.16), p=0.983 |
| None | 51 (79.7) | 13 (20.3) | Ref. | Ref. |
| cPR – Crude Prevalence Ratio; aPR – Adjusted Prevalence Ratio; CI: Confidence Interval; Ref: Reference category | ||||