Research | Open Access | Volume 9 (Suppl 12): Article 07 | Published: 14 July 2026

Views: 39
Menu, Tables and Figures
| Country | No. of Suspected Cases (2020–2024) | No. of Confirmed Cases | Total Number of Deaths | Case Fatality Rate % (CFR) |
|---|---|---|---|---|
| Nigeria | 38,900 | 5,345 | 976 | 18.3 |
| Sierra Leone | 1,575 | 64 | 43 | 67.2 |
| Liberia | 1,001 | 244 | 90 | 36.9 |
| Ghana | 494 | 28 | 1 | 3.6 |
| Guinea | 234 | 32 | 19 | 59.4 |
| Togo | 96 | 3 | 1 | 33.3 |
| Gambia | 1 | 0 | 0 | N/A |
| Côte d’Ivoire | 0 | 0 | 0 | N/A |
| Senegal | 0 | 0 | 0 | N/A |
| Benin | N/A | N/A | N/A | N/A |
| Total | 42,301 | 5,716 | 1,130 | 19.8 |
N/A = Data not available.
Table 1: Description of Lassa Fever Morbidity and Mortality Burden in the ECOWAS region (2020-2024)
Table 2: Lassa fever case diagnosis
| Country | Standard Case Definition | Case Management Guidelines | Early Warning System | Rapid Response Team | No. of RT-PCR Labs | Functional Labs | Avg. Turnaround Time (Hrs) |
|---|---|---|---|---|---|---|---|
| Nigeria | ✅ | ✅ | ✅ | ✅ | 13 | 13 | 66 hrs |
| Ghana | ✅ | ❌ | ✅ | ❌ | 1 | 1 | 108 hrs |
| Sierra Leone | ✅ | ✅ | ✅ | ✅ | 1 | 1 | 24 hrs |
| Cote d’Ivoire | ✅ | ✅ | ✅ | ✅ | 2 | 2 | 2 hrs |
| Togo | ✅ | ❌ | ✅ | ✅ | 1 | 1 | 24 hrs |
| Guinea | ✅ | ✅ | ✅ | ✅ | 6 | 6 | 15 hrs |
| Gambia | ❌ | ❌ | ❌ | ✅ | N/A | N/A | N/A |
| Liberia | ✅ | ✅ | ✅ | ✅ | 1 | 1 | 48 hrs |
| Senegal | ✅ | ✅ | ✅ | ❌ | 3 | 3 | 72 hrs |
| Benin | ✅ | ✅ | ✅ | ✅ | 2 | 2 | 14 hrs |
(✅ = Yes, ❌ = No, N/A = Not available Data)
Table 2: Lassa Fever Case Diagnosis
Table 3: Lassa fever case management availability
| Country | No. of Treatment /Isolation Centres | Ribavirin Availability | ICU Support | Contact tracing | Referral system | Contingency stockpiles of supplies. |
|---|---|---|---|---|---|---|
| Nigeria | 30 | ✅ | ✅ | ✅ | ✅ | ✅ |
| Ghana | ❌ | ❌ | ✅ | ✅ | ✅ | ❌ |
| Sierra Leone | 1 | ✅ | ✅ | ✅ | ✅ | ✅ |
| Cote d’Ivoire | ❌ | ❌ | ✅ | ✅ | ✅ | ✅ |
| Togo | ❌ | ❌ | ✅ | ✅ | ✅ | ✅ |
| Guinea | 33 | ✅ | ✅ | ✅ | ✅ | ✅ |
| Gambia | N/A | N/A | N/A | ✅ | ❌ | ✅ |
| Liberia | 8 | ✅ | ✅ | ✅ | ✅ | ✅ |
| Senegal | ❌ | ❌ | ✅ | ✅ | ✅ | ✅ |
| Benin | 3 | ✅ | ❌ | ❌ | ✅ | ✅ |
(✅ = Yes, ❌ = No, N/A = No available Data)
Table 3: Lassa fever Case management Availability
Table 4: Training and capacity building
| Country | LF Training on Case Management (months) | LF Training on IPC (months) |
|---|---|---|
| Nigeria | 12 (annually) | 12 (annually) |
| Ghana | 0 | 0 |
| Cote d’Ivoire | 0 | 0 |
| Seirra Leone | 3 (quarterly) | 3 (quarterly) |
| Togo | 0 | 0 |
| Guinea | 3(quarterly) | 3 (quarterly) |
| Gambia | N/A | N/A |
| Liberia | 0 | 0 |
| Senegal | 0 | 0 |
| Benin | 12 (annually) | 12 (annually) |
Table 4: Training and Capacity building

Kuassi Virgil Lokossou1, Andrew Sime Awori1,&, Aishat Usman1, Audu Onyemocho2, Winifred Sandra Ukponu3, Lionel Sogbossi1, Kehinde Ogunyemi4, Issiaka Sombie1, Melchior Athanase Aïssi1
1West Africa Health Organization, Abidjan, Cote d’Ivoire, 2Federal University of Health Sciences of Otukpo, Benue State, Nigeria, 3Georgetown Global Health Nigeria, Abuja, Nigeria, 4University of Georgia College of Public Health, Atlanta, Georgia, USA
&Corresponding author: Andrew Sime Awori, West Africa Health Organization, Abidjan, Côte d’Ivoire, Email: andrewaworis@gmail.com ORCID: https://orcid.org/0009-0007-1634-5504
Received: 21 Oct 2025, Accepted: 23 Mar 2026, Published: 14 Jul 2026
Domain: Infectious Disease Epidemiology
Keywords: Lassa Fever, Case Management, ECOWAS, Public Health Preparedness, Viral Hemorrhagic Fever
©Andrew Sime Awori et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Andrew Sime Awori et al., Lassa fever case management capacity in ECOWAS Region: Progress, gaps, and policy recommendations. Journal of Interventional Epidemiology and Public Health. 2026; 9(Suppl 12):07. https://doi.org/10.37432/jieph-d-25-00250
Introduction: Lassa fever remains a significant public health concern in the ECOWAS region. Prompt diagnosis and effective case management are critical for controlling outbreaks and reducing associated mortality and severe complications. This study assessed the case management capacity for Lassa fever across ECOWAS member states, focusing on early detection, diagnostics, treatment infrastructure, and infection prevention and control (IPC) measures.
Methods: A cross-sectional, mixed-methods study was conducted using structured questionnaires, key informant interviews, and document reviews in 10 ECOWAS member states. The evaluation encompassed diagnostic capacities, treatment availability, IPC measures, and workforce readiness. Thematic and comparative analyses were employed to synthesize the findings.
Results: Considerable differences were observed across participating Member States. Nigeria, Guinea, and Liberia demonstrated relative strengths in diagnostics and treatment infrastructure. In contrast, countries such as Gambia, Ghana, and Côte d’Ivoire exhibited serious shortcomings, revealing significant deficiencies in healthcare worker training and access to antiviral therapies. The implementation of standardised case management protocols was inconsistent. Additionally, data sharing challenges and inadequate coordination across borders were highlighted as significant issues.
Conclusion: While progress has been made, substantial gaps remain in Lassa fever case management across ECOWAS. Strategic investments in health systems strengthening, legal frameworks development for data sharing, and capacity building are critical to improving regional preparedness and reducing the risk of future outbreaks.
Lassa fever (LF) is a zoonotic disease caused by the Lassa virus, which belongs to the Arenaviridae family and the genus Arenavirus. The disease is endemic in West Africa, particularly in countries such as Bénin, Guinea, Liberia, Nigeria, and Sierra Leone, where it poses a significant public health threat. The reservoir host for the virus is the Mastomys natalensis rodent, which sheds the virus in its urine and feces. Humans acquire the infection through direct contact with infected rodent urine or excreta or bodily fluids of an infected individual [1].
Lassa fever manifests in a wide range of symptoms, varying from mild febrile illness to severe hemorrhagic manifestations and multi-organ failure [2]. Early symptoms are nonspecific and may include fever, headache, malaise, and sore throat, which often make it difficult to differentiate from other febrile illnesses such as malaria or typhoid fever, resulting in high missed cases or delayed diagnosis and treatment that could increase the likelihood of further community spread and poor prognosis [3]. More so, as the disease progresses, patients may develop hemorrhagic symptoms, liver and kidney dysfunction, and in severe cases, shock and death. The case fatality rate (CFR) of Lassa fever varies, ranging from 15-29.7% in hospitalized patients, with higher rates in those with severe hemorrhagic manifestations [4,5]. Early diagnosis through laboratory testing, including Real-Time Polymerase Chain Reaction (RT- PCR) assays and rapid antigen detection, is crucial for effective management and improved clinical outcomes [5].
Lassa fever shares many clinical features with other viral hemorrhagic fevers (VHFs) such as Ebola, Marburg, and Crimean-Congo hemorrhagic fever (CCHF). These diseases are similar in that they are characterized by high mortality rates, primarily due to multi-organ failure, disseminated intravascular coagulation, and shock [7]. While Ebola and Marburg are primarily transmitted through human-to-human contact, Lassa fever is unique for its transmission from rodent to human, with a higher risk due to the prevalent practices of bush burning, hunting, open-air grain storage, inadequate water, sanitation, and hygiene (WASH) systems, and poor waste disposal that increase the probability of human contact with infected rodents, particularly in rural and semi-urban areas, which pose major challenges for prevention and control [8]. Epidemiological trends from national surveillance agencies (e.g., Nigeria Centre for Disease Control) consistently show that weekly case counts rise sharply (during the dry seasons) from late November, peak in January or February, and decline around April to May. For instance, over 70% of annual confirmed Lassa cases in Nigeria typically occur between January and March [8]
Management strategies for viral hemorrhagic fevers (VHFs) share common foundational elements, particularly in relation to supportive care and infection prevention and control. Within this broader framework, the case management of Lassa fever relies primarily on early recognition, prompt supportive care, including fluid and electrolyte management and oxygen therapy, and timely administration of antiviral treatment where indicated. Ribavirin remains the most widely used antiviral for Lassa fever and has been associated with improved outcomes when administered early in the course of illness, particularly within the first six days of symptom onset. Early observational data reported reductions in mortality of approximately 56–60%; however, these estimates derive from early non-randomized studies and should be interpreted with caution. Evidence regarding ribavirin’s effectiveness remains mixed, with systematic reviews identifying significant methodological limitations, uncertainties around optimal dosing regimens, potential adverse effects in specific patient groups, and ongoing debate regarding its broader clinical benefit [9,10].
Although hemorrhagic manifestations are a defining feature of VHFs, their occurrence and severity vary considerably by disease. In Lassa fever, overt bleeding is relatively uncommon and typically less severe, underscoring the importance of focusing case management capacity on early detection, supportive care, and clinical monitoring rather than on hemorrhagic complications alone [11].
Lassa fever’s impact goes far beyond acute mortality. Long-term complications, particularly irreversible hearing loss, neurological impairment, and psychological distress, underscore the need for a comprehensive, multidisciplinary approach to management. This includes not only early diagnosis and acute care but also post-recovery support, rehabilitation services, and social protection mechanisms for survivors and their families. Recognising and addressing the full spectrum of Lassa fever’s severity is critical for shaping appropriate policies, resource allocation, and survivor-centred care strategies in endemic regions [12,13].
Given the cross-border nature of Lassa fever transmission in West Africa, effective regional coordination is critical for rapid outbreak response and control. Lessons learned from the 2014-2016 Ebola outbreak in West Africa emphasize the importance of collaborative efforts among neighboring countries in surveillance, case management, and resource allocation [14]. The establishment of a regional Lassa fever task force could significantly improve early detection, containment strategies, and outbreak management.
Enhanced cooperation through regional bodies such as the West African Health Organization (WAHO), along with other international and regional organizations could promote the sharing of resources, training of healthcare workers, and the implementation of coordinated public health campaigns. This approach could also strengthen the capacity of national healthcare systems to effectively respond to Lassa fever and other emerging infectious diseases [15].
Study design
This study employed a cross-sectional, descriptive, mixed-methods design using a convergent approach to assess Lassa fever case management capacity across selected ECOWAS Member States. Quantitative and qualitative data were collected in parallel and integrated during interpretation to provide a comprehensive assessment of health system preparedness. The study focused on institutional and system-level capacity rather than individual patient outcomes.
Study setting and population
The study was conducted in ten ECOWAS Member States selected based on Lassa fever endemicity, reporting status, and participation in regional surveillance initiatives. The unit of analysis was the country, with all findings aggregated at national level. The study population consisted exclusively of key informants and institutional data sources, including public health officials responsible for surveillance and outbreak response, clinicians involved in Lassa fever case management, laboratory focal persons, and representatives of Ministries of Health, National Public Health Institutes, and the West African Health Organization (WAHO). Patients were not interviewed, and no individual-level clinical data were collected. Only participants who provided institutional data and who were professionally involved in Lassa fever surveillance, diagnosis, treatment, infection prevention and control, or coordination were included in the interview.
Data sources and data collection
Data were collected between January 2020 and December 2024 from three sources: (1) secondary aggregated epidemiological surveillance data from national reports; (2) structured questionnaires (in French and English languages) administered to Ministries of Health and designated treatment centers covering diagnostics, treatment infrastructure, trained personnel availability, IPC, referral systems, and coordination mechanisms; and (3) semi-structured key informant interviews conducted with purposively selected officials and experts.
Data quality assurance
Data quality was ensured through cross-validation of surveillance reports, verification of questionnaire responses, triangulation of quantitative and qualitative findings, and explicit reporting of missing or unavailable data without imputation.
Data analysis
Quantitative data were analyzed descriptively using Microsoft Excel. Case fatality rates were calculated using reported deaths divided by confirmed cases with explicit denominators. Qualitative data were analyzed thematically using structured manual coding aligned with study objectives.
Ethical Considerations
The study adhered to ethical standards for human research. Ethical approval was obtained from the Institutional Review Boards (IRBs) of participating health institutions. Written informed consent was obtained from all participants, and confidentiality was assured throughout the data collection and analysis process. The study ensured that no personally identifiable information was collected and that all data were anonymised for analysis.
Between 2020 and 2024, ECOWAS countries reported over 5,700 confirmed cases of Lassa fever. Nigeria accounted for 5,345 cases, which represents 93.5% of the total confirmed cases, followed by Liberia (4.3%), Sierra Leone (1.1%), Guinea (0.55%), Ghana (0.5%), and Togo (0.05%). The overall regional death recorded were 1130 and a case fatality rate (CFR) of 20.0%. However, the CFR varied across different countries, with Sierra Leone and Guinea reporting higher rates of 67% and 59%, respectively. Other countries showed the following CFRs: Liberia at 37.0%, Togo at 33.0%, Nigeria at 18.0%, and Ghana at 3.6%.
Human resources for Lassa fever case management
Availability of trained personnel for Lassa fever case management varied substantially across the ten ECOWAS Member States. Nigeria and Benin reported the presence of clinicians, laboratory scientists, and IPC focal persons who received structured and periodic training on Lassa fever case management. In contrast, Ghana, Senegal, Liberia, and Côte d’Ivoire reported no routine or formalised training programs during the assessment period, relying instead on ad-hoc orientation during outbreaks. Some countries reported shortages of trained laboratory personnel capable of handling viral hemorrhagic fever diagnostics, particularly outside capital cities.
Lassa fever endemicity and reporting status
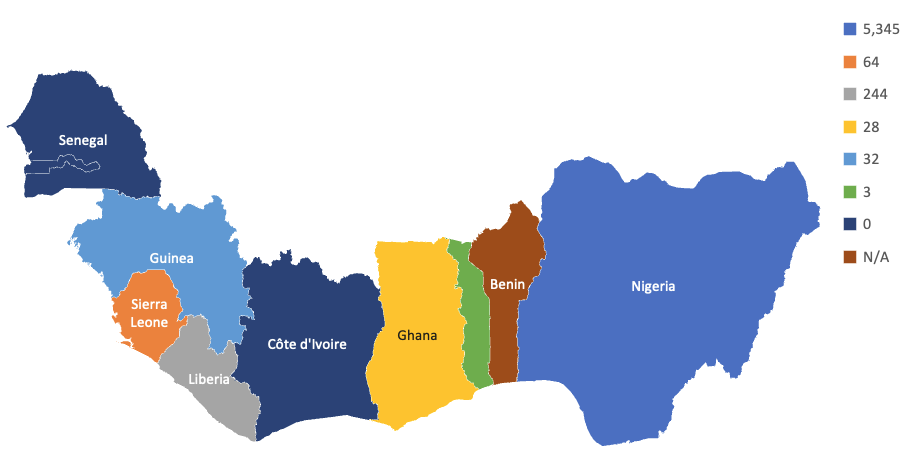
Among the ten ECOWAS Member States assessed, Nigeria, Sierra Leone, Liberia, Guinea, and Benin were classified as endemic countries with either regular or historical reporting of confirmed Lassa fever cases. Ghana, Togo, and The Gambia reported sporadic or imported cases, while Côte d’Ivoire and Senegal reported no confirmed cases during the study period. The distribution of Lassa fever cases varies across countries in the region. Figure 1 shows the geographic distribution of confirmed cases of Lassa fever across the ECOWAS region between 2020 and 2024. Countries with limited or no reporting also demonstrated weaker surveillance systems and limited diagnostic capacity, suggesting potential under-detection of cases rather than the true absence of disease.
Diagnostic capacity
Sierra Leone was confirmed to have national diagnostic capacity for Lassa fever at Kenema Government Hospital, which functions as a reference laboratory with RT-PCR testing capability and an average turnaround time of approximately 24 hours. This capacity complements existing diagnostic infrastructure in Nigeria, Guinea, Liberia, and Côte d’Ivoire, while several other countries continue to rely on external referral laboratories. However, diagnostic capacity remains highly centralized, with most advanced testing facilities located in capital cities or national reference laboratories. Subnational health facilities, particularly in rural areas, often lack on-site diagnostic capability and depend on sample referral systems. This challenge is exacerbated by shortages of trained laboratory personnel capable of handling viral hemorrhagic fever diagnostics outside major urban centers. Consequently, delays in sample transport and result turnaround times at subnational levels may limit the effectiveness of surveillance systems and delay timely case management and outbreak response.
Treatment infrastructure and supportive care
Treatment capacity across the ECOWAS region was unevenly distributed. Guinea and Nigeria had the highest number of treatment/isolation centres (33 and 30, respectively), while Liberia had moderate capacity (eight centres). In contrast, countries such as Ghana, Senegal, Côte d’Ivoire, and Togo lacked designated treatment centres and relied on temporary repurposing of general wards. Sierra Leone reported only one treatment facility despite relatively strong ICU support.
As shown in Table 3, access to Ribavirin remained inconsistent, particularly in countries without established treatment centres. ICU capacity was available in Nigeria, Guinea, Liberia, and Sierra Leone but was limited or absent in others, including Benin. Although most countries reported functional contact tracing and referral systems, gaps persisted in contingency stockpiles and critical care capacity.
Overall, these findings highlight significant regional disparities in case management capacity, particularly at the subnational level. Strengthening decentralized treatment infrastructure, ensuring consistent availability of essential therapeutics, and expanding critical care capacity are essential to improving timely case management and outbreak response.
Training and preparedness for infection prevention and control (IPC)
Structured training for managing Lassa fever cases was not consistently implemented. Nigeria and Benin had comprehensive, year-long training initiatives targeting infectious disease clinicians and IPC focal persons. In contrast, most of the other countries, including Ghana, Senegal, and Liberia, lacked formal curricula and periodic refresher training
Coordination and data sharing
National referral systems and cross-border coordination are still undeveloped. Weak surveillance systems, language barriers, and a lack of interoperable digital platforms hinder the timely exchange of data. Only a few countries utilize digital disease surveillance platforms like the surveillance outbreak response management and analysis system (SORMAS) in Nigeria or electronic integrated disease surveillance and response (e-IDSR) hosted on the District Health Information System (DHIS 2) in Liberia, Sierra Leone and Ghana. Additionally, Legal and regulatory frameworks governing data sharing are fragmented or absent in several states, complicating regional outbreak response.
This study provides a regional overview of Lassa fever case management capacity across selected ECOWAS Member States and reveals substantial heterogeneity in diagnostic capacity, availability of trained personnel, treatment infrastructure, and surveillance systems.
Observed disparities in diagnostic capacity across ECOWAS Member States point to underlying structural differences in laboratory networks and surveillance systems. Countries with regular reporting of Lassa fever cases, such as Nigeria, Sierra Leone, Guinea, Liberia, and Benin, demonstrated comparatively stronger diagnostic infrastructure and greater institutional experience with case detection and confirmation. In contrast, countries reporting sporadic or no cases frequently exhibited limited laboratory coverage, longer diagnostic turnaround times, and reliance on external referral laboratories [18,19].
Rather than indicating lower transmission risk, these patterns likely reflect surveillance and reporting biases, whereby limited access to diagnostics reduces case detection and confirmation. In peripheral health facilities, febrile illnesses are often managed syndromically, increasing the likelihood that Lassa fever cases are misclassified as malaria or typhoid fever [18]. Such under-detection may, in turn, contribute to lower prioritisation of Lassa fever within national health agendas, reinforcing a cycle of limited investment in diagnostic capacity. Similar dynamics have been reported in other Lassa-endemic settings where weak surveillance obscures the true burden of disease [19].
From a health systems perspective, these findings correspond to gaps within the WHO health system building blocks, particularly service delivery and health information systems. Strengthening decentralized diagnostics, integrating Lassa fever into routine febrile illness algorithms, and improving laboratory–surveillance linkages have been recommended as critical strategies for improving early detection and response [18,19].
Differences in treatment infrastructure across ECOWAS Member States reflect broader health system constraints rather than isolated deficiencies in Lassa fever care. Access to ribavirin and the capacity to provide essential supportive care—including oxygen therapy, renal support, and safe isolation—were unevenly distributed across the region. While delayed or inconsistent access to antiviral therapy and supportive care may contribute to poorer outcomes, this study does not establish direct causal relationships between infrastructure gaps and mortality.
Nevertheless, existing evidence indicates that early administration of ribavirin, ideally within the first six days of illness, is associated with improved survival in Lassa fever, although its effectiveness remains subject to methodological limitations and ongoing debate [9,10]. Variability in access to antivirals and supportive care therefore highlights differences in health system readiness, including supply chain reliability and facility-level capacity to implement recommended treatment protocols. These findings are consistent with prior studies emphasizing that effective Lassa fever management depends not only on antiviral availability but also on timely diagnosis, clinical monitoring, and infection prevention and control measures [24,25].
Human resource capacity emerged as a recurrent constraint across multiple domains of Lassa fever case management. Countries reporting structured and recurrent training programs appeared better positioned to implement standard case definitions, infection prevention and control measures, and treatment protocols. Conversely, reliance on ad-hoc, outbreak-driven training approaches may undermine continuity of care and increase occupational risk for healthcare workers, as documented in previous outbreak settings [24,26].
These patterns reflect broader challenges within the health workforce building block, particularly in relation to training institutionalisation and workforce retention. While this study did not assess training effectiveness or competency outcomes, the findings support existing recommendations advocating for the integration of Lassa fever competencies into routine pre-service and in-service training programs rather than episodic response-focused capacity building [25,26].
The study also highlights persistent weaknesses in regional coordination, including fragmented legal frameworks, limited interoperability of surveillance platforms, and delayed cross-border information exchange. Given the endemic and transboundary nature of Lassa fever, such systemic constraints may hinder timely outbreak detection and coordinated response efforts, as previously reported in the region [25].
These challenges align with gaps in the leadership and governance and health information systems building blocks. Strengthening regional governance mechanisms under ECOWAS and the West African Health Organization could facilitate harmonized protocols, shared surveillance platforms, and coordinated deployment of resources. Lessons from prior regional public health emergencies underscore the importance of governance and political commitment in enabling effective cross-border collaboration [25,28].
Although Lassa fever shares certain clinical features with other viral hemorrhagic fevers, this study deliberately focused on Lassa fever case management due to its distinct epidemiology, transmission dynamics, and endemicity within West Africa [31]. References to other VHFs are intended solely to contextualize shared health system challenges rather than to directly compare disease-specific response capacity, thereby avoiding conflation of management requirements across different pathogens.
Lessons and implications
Taken together, the findings suggest that observed gaps in Lassa fever case management capacity across ECOWAS Member States are best understood as manifestations of broader health system constraints rather than isolated technical failures. Addressing these gaps will likely require coordinated investments across multiple health system building blocks, including diagnostics, workforce development, surveillance systems, and regional governance [15,25]. While causal inferences cannot be drawn from this study, the patterns identified provide actionable insights for strengthening preparedness and response in Lassa fever–endemic and at-risk settings.
Policy and research implications
This study highlights urgent priorities for policy and research priorities. From a policy perspective, the creation of a regional task force for LF should be prioritized to centralize the coordination of diagnostic and treatment standards, facilitate resource pooling, and lead emergency preparedness planning. National governments must also invest in surveillance systems, particularly in underserved and border regions, to support early outbreak detection.
Longitudinal studies on LF transmission dynamics, especially in peri-urban and conflict-affected zones, are essential to effectively tailor control strategies.
Limitations
Despite the regional scope of this assessment, important limitations should be considered when interpreting the findings. The cross-sectional design allows identification of system-level patterns but does not support causal inference between case management capacity and patient outcomes. Reported differences in Lassa fever burden across countries are therefore likely influenced by variability in surveillance sensitivity, diagnostic availability, and reporting practices, particularly in settings with limited laboratory capacity where under-detection is probable.
The study draws on secondary quantitative data and qualitative inputs from public health officials, which introduces uncertainty related to data completeness and potential informant bias. While triangulation across data sources was undertaken, perspectives on preparedness and coordination may reflect institutional viewpoints rather than objective performance metrics. In addition, heterogeneity in data availability across countries limited the precision of some indicators, including workforce capacity and case fatality estimates. These constraints highlight the need for standardized data collection and longitudinal designs in future regional assessments.
Policy Recommendations
This study underscores the urgent need for a multifaceted approach to LF management in West Africa. Key recommendations include:
By addressing gaps in diagnostic, therapeutic, and coordination, ECOWAS countries can mitigate the impact of LF and build resilient health systems capable of managing future outbreaks. The lessons learned from LF are also applicable to other emerging infectious diseases, reinforcing the importance of regional collaboration in global health security.
This study provides a descriptive regional assessment of Lassa fever case management capacity across selected ECOWAS Member States and highlights marked heterogeneity in diagnostics, availability of trained personnel, treatment infrastructure, and surveillance systems. The findings suggest that countries reporting few or no Lassa fever cases often have more limited diagnostic reach and surveillance sensitivity, indicating that under-detection rather than true absence of disease may contribute to lower reported burden.
While progress has been observed in a subset of endemic countries with established diagnostic and treatment capacity, overall preparedness for Lassa fever across the region remains uneven. Given the cross-sectional nature of the study, these observations should be interpreted as reflecting system-level capacity patterns rather than direct determinants of patient outcomes. Nonetheless, the identified gaps underscore the importance of strengthening core health system functions that support early detection, appropriate case management, and safe care delivery.
Within these constraints, the findings point to potential areas for improvement, including expanded access to decentralized diagnostics, more consistent institutionalized training for healthcare workers, strengthened surveillance systems, and improved coordination across national and regional levels. The role of regional platforms, particularly the West African Health Organization, may be relevant in facilitating harmonization of case management standards, information sharing, and collective preparedness efforts, while recognizing that the effectiveness of such approaches warrants further evaluation.
Future research using longitudinal designs, standardized primary data collection, and robust clinical and operational studies would be valuable for better understanding the impact of specific interventions, including antiviral use, supportive care models, and surveillance strengthening, on Lassa fever outcomes. Strengthening the evidence base in these areas will be essential for informing targeted and context-appropriate strategies to reduce the burden of Lassa fever and enhance regional health security.
What is already known about the topic
What this study adds
The authors gratefully acknowledge the support of the West African Health Organization (WAHO) for its leadership in coordinating this regional assessment. We also extend our sincere appreciation to the Directors of Public Health, National Public Health Institutes, and other key stakeholders across the ECOWAS Member States for their invaluable contributions and participation in the readiness assessment. Lastly, we acknowledge the contributions of administrative and technical staff who supported data collection, analysis, and manuscript preparation. Their efforts were critical to the successful completion of this work.
VL led the overall study design. AA coordinated data collection efforts across ECOWAS Member States, data analysis and interpretation, as well as manuscript drafting. VF, AU, LS, OA, UW, and OK, oversaw data analysis and interpretation, provided technical inputs, and participated in manuscript review. IS and MA supervised the study, contributed to the interpretation of results, and provided an overall editorial review. All authors have reviewed and approved the final version of the manuscript.
| Country | No. of Suspected Cases (2020–2024) | No. of Confirmed Cases | Total Number of Deaths | Case Fatality Rate % (CFR) |
|---|---|---|---|---|
| Nigeria | 38,900 | 5,345 | 976 | 18.3 |
| Sierra Leone | 1,575 | 64 | 43 | 67.2 |
| Liberia | 1,001 | 244 | 90 | 36.9 |
| Ghana | 494 | 28 | 1 | 3.6 |
| Guinea | 234 | 32 | 19 | 59.4 |
| Togo | 96 | 3 | 1 | 33.3 |
| Gambia | 1 | 0 | 0 | N/A |
| Côte d’Ivoire | 0 | 0 | 0 | N/A |
| Senegal | 0 | 0 | 0 | N/A |
| Benin | N/A | N/A | N/A | N/A |
| Total | 42,301 | 5,716 | 1,130 | 19.8 |
N/A = Data not available.
| Country | Standard Case Definition | Case Management Guidelines | Early Warning System | Rapid Response Team | No. of RT-PCR Labs | Functional Labs | Avg. Turnaround Time (Hrs) |
|---|---|---|---|---|---|---|---|
| Nigeria | ✅ | ✅ | ✅ | ✅ | 13 | 13 | 66 hrs |
| Ghana | ✅ | ❌ | ✅ | ❌ | 1 | 1 | 108 hrs |
| Sierra Leone | ✅ | ✅ | ✅ | ✅ | 1 | 1 | 24 hrs |
| Cote d’Ivoire | ✅ | ✅ | ✅ | ✅ | 2 | 2 | 2 hrs |
| Togo | ✅ | ❌ | ✅ | ✅ | 1 | 1 | 24 hrs |
| Guinea | ✅ | ✅ | ✅ | ✅ | 6 | 6 | 15 hrs |
| Gambia | ❌ | ❌ | ❌ | ✅ | N/A | N/A | N/A |
| Liberia | ✅ | ✅ | ✅ | ✅ | 1 | 1 | 48 hrs |
| Senegal | ✅ | ✅ | ✅ | ❌ | 3 | 3 | 72 hrs |
| Benin | ✅ | ✅ | ✅ | ✅ | 2 | 2 | 14 hrs |
| Country | No. of Treatment /Isolation Centres | Ribavirin Availability | ICU Support | Contact tracing | Referral system | Contingency stockpiles of supplies. |
|---|---|---|---|---|---|---|
| Nigeria | 30 | ✅ | ✅ | ✅ | ✅ | ✅ |
| Ghana | ❌ | ❌ | ✅ | ✅ | ✅ | ❌ |
| Sierra Leone | 1 | ✅ | ✅ | ✅ | ✅ | ✅ |
| Cote d’Ivoire | ❌ | ❌ | ✅ | ✅ | ✅ | ✅ |
| Togo | ❌ | ❌ | ✅ | ✅ | ✅ | ✅ |
| Guinea | 33 | ✅ | ✅ | ✅ | ✅ | ✅ |
| Gambia | N/A | N/A | N/A | ✅ | ❌ | ✅ |
| Liberia | 8 | ✅ | ✅ | ✅ | ✅ | ✅ |
| Senegal | ❌ | ❌ | ✅ | ✅ | ✅ | ✅ |
| Benin | 3 | ✅ | ❌ | ❌ | ✅ | ✅ |
| Country | LF Training on Case Management (months) | LF Training on IPC (months) |
|---|---|---|
| Nigeria | 12 (annually) | 12 (annually) |
| Ghana | 0 | 0 |
| Cote d’Ivoire | 0 | 0 |
| Seirra Leone | 3 (quarterly) | 3 (quarterly) |
| Togo | 0 | 0 |
| Guinea | 3(quarterly) | 3 (quarterly) |
| Gambia | N/A | N/A |
| Liberia | 0 | 0 |
| Senegal | 0 | 0 |
| Benin | 12 (annually) | 12 (annually) |