Research | Open Access | Volume 9 (2): Article 105 | Published: 22 Jun 2026
Views: 25
Menu, Tables and Figures
| Variable | Frequency (n=1,438) | Percentage (%) |
|---|---|---|
| Age (years) | ||
| 18–29 | 575 | 40 |
| 30–44 | 560 | 39 |
| 45–59 | 213 | 15 |
| ≥60 | 90 | 6 |
| Sex | ||
| Female | 614 | 43 |
| Male | 824 | 57 |
| Marital status | ||
| Married | 621 | 43 |
| Separated | 42 | 3 |
| Single | 600 | 42 |
| Widow(er) | 193 | 13 |
| Level of education | ||
| None | 79 | 5 |
| Primary | 463 | 32 |
| Secondary | 638 | 44 |
| Tertiary | 258 | 18 |
| Occupation | ||
| Business | 832 | 58 |
| Formal employment | 244 | 17 |
| None | 325 | 23 |
| Casual laborer | 37 | 2 |
| Region | ||
| Central | 659 | 46 |
| Eastern | 306 | 21 |
| Northern | 93 | 6 |
| Western | 380 | 26 |
Table 1: Socio-demographic characteristics of pilgrims during the Martyrs Day commemoration event, Uganda, May 29–June 4, 2025, n=1,438
| Variable | Knowledge | cPR (95% CI) | aPR (95% CI) | |
|---|---|---|---|---|
| Good n (%) n=575 | Poor n (%) n=863 | |||
| Age (years) | ||||
| 18–29 | 210 (37) | 365 (63) | Ref | Ref |
| 30–44 | 250 (45) | 310 (55) | 1.22 (1.10–1.35) | 1.10 (1.02–1.15) |
| 45–59 | 180 (85) | 33 (15) | 2.32 (2.10–2.56) | 2.40 (1.80–3.10) |
| ≥60 | 36 (40) | 54 (60) | 1.10 (0.90–1.34) | 1.00 (0.85–1.18) |
| Sex | ||||
| Female | 230 (38) | 384 (62) | Ref | Ref |
| Male | 340 (41) | 484 (59) | 1.10 (1.01–1.21) | 1.10 (1.02–1.20) |
| Education | ||||
| None | 10 (13) | 69 (87) | Ref | Ref |
| Primary | 122 (26) | 341 (74) | 2.08 (1.20–3.60) | 2.70 (1.90–3.90) |
| Secondary | 180 (28) | 458 (72) | 2.22 (1.30–3.80) | 6.10 (4.50–8.20) |
| Tertiary | 65 (25) | 193 (75) | 1.98 (1.10–3.50) | 7.20 (5.20–9.80) |
| Ref: Reference; cPR: crude Prevalence Ratio; aPR: adjusted Prevalence Ratio; CI: confidence interval | ||||
Table 2: Factors associated with knowledge of mpox among pilgrims, Uganda, May 29–June 4, 2025, n=1,438
| Variable | Attitude | cPR (95% CI) | aPR (95% CI) | |
|---|---|---|---|---|
| Yes (n, %) n=576 | No (n, %) n=862 | |||
| Age (years) | ||||
| 18–29 | 172 (30) | 403 (70) | Ref | Ref |
| 30–44 | 319 (57) | 241 (43) | 1.91 (1.65–2.20) | 1.90 (1.30–2.70) |
| 45–59 | 64 (30) | 149 (70) | 1.00 (0.79–1.28) | 1.00 (0.60–1.60) |
| ≥60 | 24 (27) | 66 (73) | 0.89 (0.62–1.29) | 0.90 (0.50–1.50) |
| Sex | ||||
| Female | 246 (40) | 368 (60) | Ref | Ref |
| Male | 330 (40) | 494 (60) | 1.00 (0.88–1.13) | 1.00 (0.80–1.20) |
| Education | ||||
| None | 16 (20) | 63 (80) | Ref | Ref |
| Primary | 204 (44) | 259 (56) | 2.17 (1.39–3.40) | 2.20 (1.30–3.80) |
| Secondary | 447 (70) | 191 (30) | 3.45 (2.22–5.37) | 4.90 (2.70–8.90) |
| Tertiary | 206 (80) | 52 (20) | 3.93 (2.53–6.11) | 6.10 (3.30–11.10) |
| Ref: Reference; cPR: crude Prevalence Ratio; aPR: adjusted Prevalence Ratio; CI: confidence interval | ||||
Table 3: Factors associated with positive attitudes towards mpox among pilgrims, Uganda, May 29–June 4, 2025, n=1,438
| Variable | Practices | cPR (95% CI) | aPR (95% CI) | |
|---|---|---|---|---|
| Good (n, %) n=345 | Poor (n, %) n=1,093 | |||
| Age (years) | ||||
| 18–29 | 130 (23) | 445 (77) | Ref | Ref |
| 30–44 | 150 (27) | 410 (73) | 1.17 (0.93–1.47) | 1.15 (0.85–1.55) |
| 45–59 | 45 (21) | 168 (79) | 0.91 (0.66–1.27) | 0.90 (0.60–1.30) |
| ≥60 | 20 (22) | 70 (78) | 0.96 (0.61–1.51) | 0.95 (0.55–1.60) |
| Sex | ||||
| Female | 150 (24) | 464 (76) | Ref | Ref |
| Male | 195 (24) | 629 (76) | 1.00 (0.82–1.22) | 1.00 (0.75–1.30) |
| Education level | ||||
| None | 12 (15) | 67 (85) | Ref | Ref |
| Primary | 100 (22) | 363 (78) | 1.47 (0.83–2.60) | 1.40 (0.70–2.80) |
| Secondary | 170 (27) | 468 (73) | 1.80 (1.02–3.20) | 1.70 (0.90–3.20) |
| Tertiary | 63 (24) | 195 (76) | 1.60 (0.88–2.90) | 1.50 (0.70–3.10) |
| Ref: Reference; cPR: crude Prevalence Ratio; aPR: adjusted Prevalence Ratio; CI: confidence interval | ||||
Table 4: Factors associated with positive attitudes towards mpox among pilgrims, Uganda, May 29-June 4, 2025, n=1,438
Martha Dorcas Nalweyiso1,&, Justine Wobusobozi1, Aminah Namwabira1, Bernard Lubwama1, Anne Loy Alupo1, Richard Migisha1, Benon Kwesiga1, Emmanuel Obuya1, Alex Riolexus Ario1
1Uganda National Institute of Public Health, Kampala, Uganda
&Corresponding author: Martha Dorcas Nalweyiso, Uganda National Institute of Public Health, Kampala, Uganda, Email: nmartha@uniph.go.ug ORCID: https://orcid.org/0009-0008-4921-4356
Received: 13 May 2026, Accepted: 21 Jun 2026, Published: 22 Jun 2026
Domain: Infectious Disease Epidemiology
Keywords: Mpox, Knowledge, Attitude, Practices, Uganda
©Martha Dorcas Nalweyiso et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Martha Dorcas Nalweyiso et al., Knowledge, attitudes, and practices related to mpox among pilgrims at the 2025 Uganda Martyrs’ Day commemoration, Namugongo, Uganda. Journal of Interventional Epidemiology and Public Health. 2026; 9(2):105. https://doi.org/10.37432/jieph-d-26-00152
Introduction: In May 2025, Uganda reported widespread mpox transmission across most districts. Mass gatherings, such as the Martyrs’ Day Commemoration, pose heightened transmission risks. We assessed knowledge, attitudes, and practices (KAP) regarding mpox, as well as factors associated with KAP among pilgrims during the commemoration.
Methods: We conducted a cross-sectional study among pilgrims from May 29 to 4 June 2025. Using systematic intercept sampling, every tenth pilgrim entering any of the 14 shrine entry points was enrolled. Data were collected using a structured questionnaire. KAP scores were categorised using a modified Bloom’s cut-off (≥60%=adequate knowledge, positive attitude, good practice). We used modified Poisson regression to identify associated factors, reporting adjusted prevalence ratios (aPRs) and 95% confidence intervals (CIs).
Results: Among 1,438 pilgrims (median age 37 years; interquartile range [IQR]: 25–43; 58% male), 40% (95% CI: 37.5%–42.5%) had adequate knowledge, 40% (95% CI: 37.6%–42.6%) had positive attitudes, and 24% (95% CI: 21.8%–26.2%) reported good preventive practices. Awareness was high (85%), but only 25% identified vaccination as preventive. Additionally, 90% reported handwashing, 26% reported physical distancing, and 47% reported sharing personal items. Compared with pilgrims with no formal education, higher educational attainment was associated with adequate knowledge (primary: aPR=2.70; secondary: aPR=6.10; tertiary: aPR=7.20) and positive attitudes (primary: aPR=2.20; secondary: aPR=4.90; tertiary: aPR=6.10). Older age was associated with adequate knowledge (45–59 versus 18–29 years: aPR=2.40) and positive attitudes (30–44 versus 18–29 years: aPR=1.90). No factors were associated with good preventive practices.
Conclusion: Knowledge and attitudes towards mpox were moderate, but preventive practices were low. Knowledge and attitudes were associated with age and education. These findings suggest that awareness alone is insufficient to change behaviour. During public health responses, there is a need to combine targeted risk communication with enabling interventions to improve uptake of preventive measures during mass gatherings.
Mpox is a re-emerging zoonotic disease caused by the monkeypox virus that has expanded rapidly across multiple regions, including Uganda [1]. Uganda reported the onset of the current mpox outbreak in July 2024, and by May 2025, cases had been identified in most districts nationwide, indicating widespread transmission and ongoing public health risk [2, 3]. In the absence of widespread vaccination, effective prevention relies heavily on awareness and consistent adoption of protective practices [4].
Mass gatherings are recognized as high-risk environments for the transmission of infectious diseases due to crowd density, prolonged close contact, and population mixing [5]. The Uganda Martyrs’ Day commemoration, held annually on June 3 in Namugongo, attracts over two million pilgrims from across the country. Syndromic surveillance during previous events has identified symptoms consistent with infectious diseases, underscoring the potential for rapid transmission and the need for targeted prevention strategies in such settings [6]. Although previous studies in Uganda have assessed mpox-related knowledge and attitudes among healthcare workers and community groups, data from high-risk mass gathering settings remain limited [4,7]. Understanding Knowledge, Attitudes and Practices (KAP) in this context is critical to inform risk communication and community engagement strategies tailored to outbreak response.
The 2024–2025 mpox outbreak coincided with preparations for the annual Uganda Martyrs’ Day commemoration, raising concerns about potential transmission during the event [8, 9]. Because pilgrims travel from across Uganda, this mass gathering provided a unique opportunity to characterize population-level KAP related to mpox during an ongoing outbreak. Generating such evidence during a period of active transmission was critical to inform timely outbreak response, including risk communication and community engagement strategies for this and future mass gatherings. This study assessed knowledge, attitudes, and practices related to mpox and associated factors among pilgrims attending the 2025 Uganda Martyrs’ Day commemoration in Namugongo.
Study setting
The study was conducted at the Uganda Martyrs Shrine in Namugongo Town Council, Kiira Municipality, Wakiso District, during the annual Uganda Martyrs’ Day commemoration held on June 3. This event is one of the largest religious mass gatherings in Uganda, attracting hundreds of thousands of pilgrims from across the country and neighbouring countries [8, 9]. The multi-day event involves dense crowding, prolonged close contact, shared accommodation, and limited water, sanitation, and hygiene (WASH) facilities.
Study design and population
We conducted a cross-sectional assessment among pilgrims from May 29 to June 4, 2025. Eligible participants were pilgrims aged ≥18 years attending the commemoration. We excluded healthcare workers and religious leaders because of their potential involvement in mpox response activities and higher likelihood of prior exposure to health information. International pilgrims were excluded to maintain comparability with Uganda-focused outbreak response interventions.
Sample size and sampling
Because this was a rapid operational assessment conducted during a large mass gathering, no fixed sample size was prespecified. Instead, an ad hoc sample size was approximated for planning purposes, with an estimated minimum of 410 participants considered sufficient to provide stable descriptive estimates of mpox-related knowledge, attitudes, and practices. This approximation was based on standard assumptions for cross-sectional surveys, including a 60% expected prevalence of adequate knowledge from a prior study [4], a 95% confidence level, a 5% margin of error, and a 10% allowance for non-response. However, to enhance precision and maximize programmatic usefulness, all eligible consenting pilgrims encountered during the data collection period were enrolled.
We used a systematic intercept sampling approach to recruit participants at designated data collection points across both the Catholic and Anglican sections of the shrine. Research assistants positioned at major entry points approached every 10th eligible pilgrim in line, with the sampling interval guided by participant flow at each site. A random start was used at the beginning of each sampling period. If a selected pilgrim declined participation or was ineligible, the next eligible pilgrim was approached. To minimize clustering within travel groups, only one participant per identifiable group was enrolled when feasible.
Study variables and data collection
Data were collected using a structured, interviewer-administered questionnaire programmed in Kobo Collect. The tool was adapted from previously used KAP instruments for COVID-19 and Ebola, as well as the World Health Organisation’s mpox guidance [10, 11], and was pretested before implementation. The questionnaire underwent expert review to assess content validity and was pretested before implementation to ensure clarity, relevance and appropriateness of the items within the study context. Research assistants, who were master’s students in public health, were trained in study procedures, consent processes, and standardised interviewing techniques to ensure consistency in data collection. The questionnaire captured sociodemographic characteristics, including age, sex, education level, marital status, and region of origin, as well as mpox-related knowledge, attitudes, and practices. Knowledge was assessed through items on awareness, modes of transmission, symptoms, high-risk groups, and prevention measures. Attitudes included perceived risk, responsibility for prevention, willingness to report suspected cases, vaccine acceptance, and stigma towards infected individuals. Practices were assessed through reported preventive behaviours, sharing of personal items, care-seeking behaviour, and symptom reporting. Mpox was described to participants as a viral zoonotic disease transmitted through close contact with infected persons, contaminated materials, or infected animals, consistent with WHO guidance. Each KAP domain comprised 10 items, with responses scored as 1 for correct or appropriate and 0 for incorrect or inappropriate, yielding a total score ranging from 0 to 10 for each domain.
Outcome definitions
Knowledge, attitudes, and practices were categorised using a modified Bloom’s cut-off of scores ≥60% (≥6 out of 10) as adequate knowledge, positive attitude, and good practice, respectively [10]. The modified Bloom’s cut off has been widely used in KAP studies to classify adequate knowledge, positive attitudes and good practices [10]. The 60% cut-off has been used in KAP studies to provide a pragmatic outcome between adequate and inadequate outcomes. Given the varying backgrounds of pilgrims and the emergence of mpox, we considered this cut off appropriate for the study population.
Data analysis
Data were extracted from the Kobo Collect tool, cleaned in Microsoft Excel, and analysed using STATA version 17. Categorical variables were summarized using frequencies and percentages, and continuous variables were summarized using means and standard deviations. We used modified Poisson regression with robust standard errors to estimate crude prevalence ratios (cPRs) and adjusted prevalence ratios (aPRs) with 95% confidence intervals (CIs) for factors associated with adequate knowledge, positive attitudes, and good practices. Variables with p<0.2 at bivariate analysis and those considered epidemiologically relevant were included in multivariable models. Before model fitting, multicollinearity among explanatory variables was assessed using variance inflation factors, and no evidence of problematic collinearity was identified. Statistical significance was assessed at p<0.05.
Ethical considerations
The Ministry of Health, Uganda, provided administrative clearance to conduct this study and was therefore determined to be non-research. In agreement with the International Guidelines for Ethical Review of Epidemiological Studies by the Council for International Organisations of Medical Sciences (1991) and the Office of the Associate Director for Science, US CDC/Uganda, it was determined that this activity was not human subject research and that its primary intent was to improve public health practice or disease control. This activity was reviewed by the US CDC and conducted in accordance with applicable federal law and CDC policy. §§See, e.g., 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq. Permission to conduct this study was also granted by the City Health Office. Eligible participants aged 18 years and above were informed about the purpose of the study and provided voluntary informed consent before participation. To ensure confidentiality, no personal identifiers were collected, and the investigation team stored the data under password protection.
Social demographic characteristics of pilgrims during the Martyrs Day commemoration event, Uganda, May 29–June 4, 2025
Of 1,438 pilgrims enrolled between May 29 and June 4, 2025, the median age was 37 years (interquartile range [IQR], 25–43). Overall, 575 (40%) were aged 18–29 years, 560 (39%) were aged 30–44 years, 213 (15%) were aged 45–59 years, and 90 (6%) were aged ≥60 years. More than half were male (824, 54%), and 600 (42%) were single. Most participants had attained secondary education 638 (44%), 832 (58%) were engaged in business activities, and 659 (46%) originated from the central region (46%) (Table 1).
Knowledge, attitudes, and practices related to mpox
Among 1,438 participants, 575 (40%; 95% Confidence Interval (CI):37.5-42.5) had adequate knowledge of mpox, 576 (40%; 95% CI: 37.6- 42.6) had a positive attitude towards mpox prevention, and 345 (24%; 95% CI:21.8-26.2) reported good preventive practices.
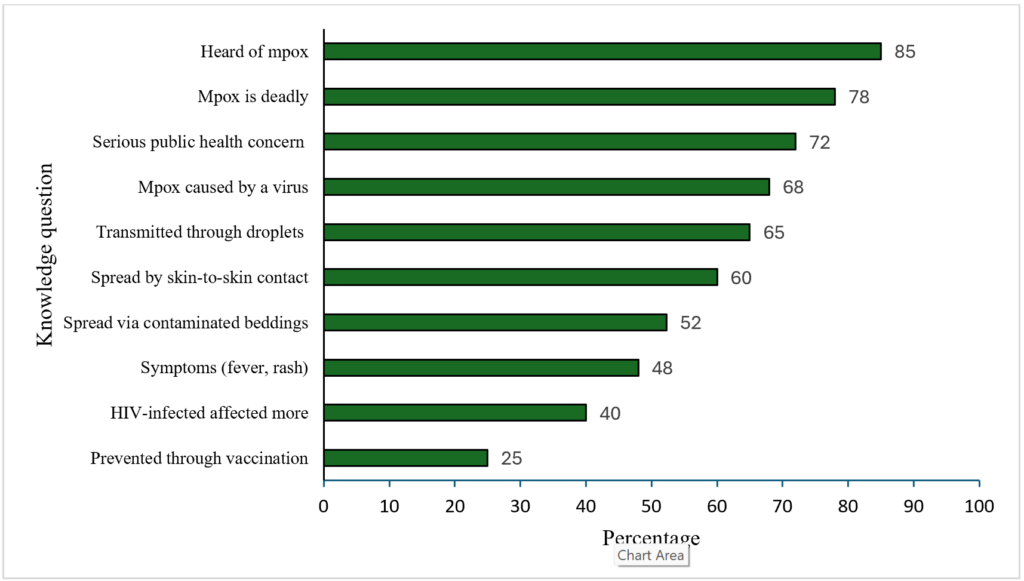
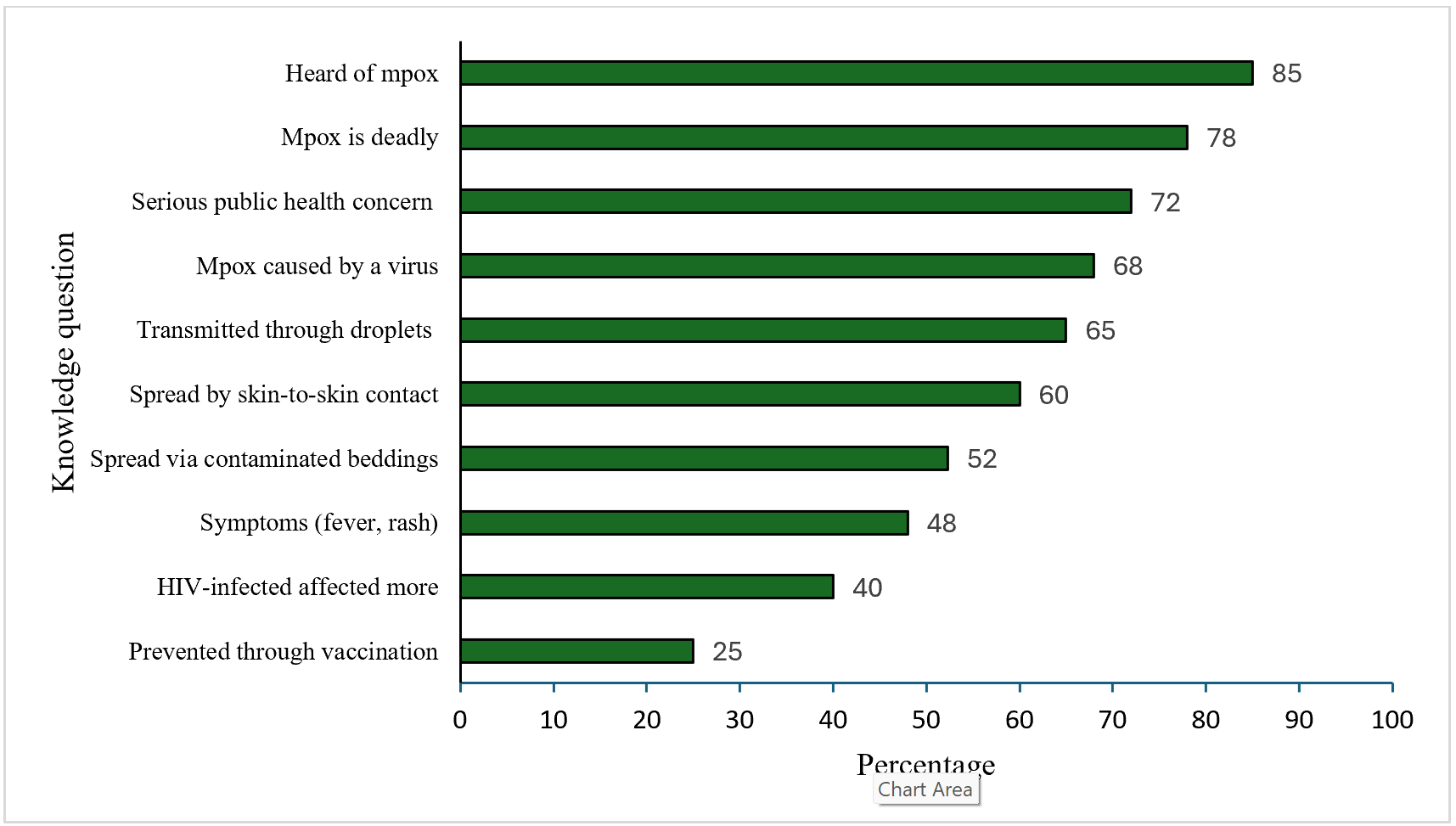
Among participants, awareness of mpox was high, with 1,222 (85%) reporting having heard of the disease. A substantial proportion, 1,035 (72%), recognized mpox as a serious public health concern and a severe disease, 1,122 (78%), while 978 (68%) correctly identified it as a viral infection. Knowledge of transmission routes was moderate: 935 (65%) identified respiratory droplets, 863 (60%) recognized skin-to-skin contact with lesions, and 748 (52%) identified contaminated bedding. Recognition of key symptoms (fever, rash, and lymphadenopathy) was reported by 690 (48%). Knowledge gaps were evident; only 575 (40%) recognized increased risk among persons living with HIV, and 360 (25%) identified vaccination as a preventive measure (Figure 1).
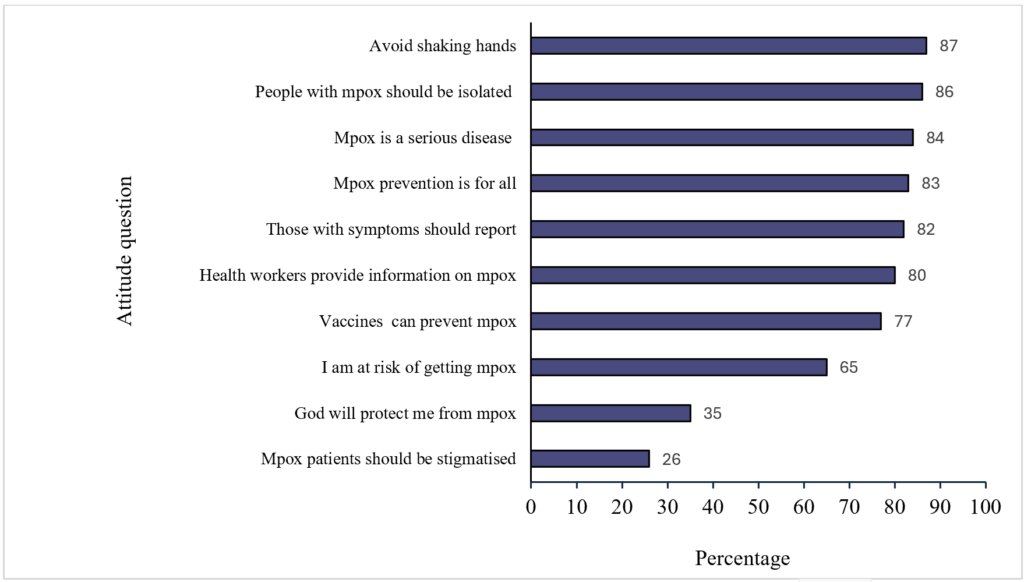
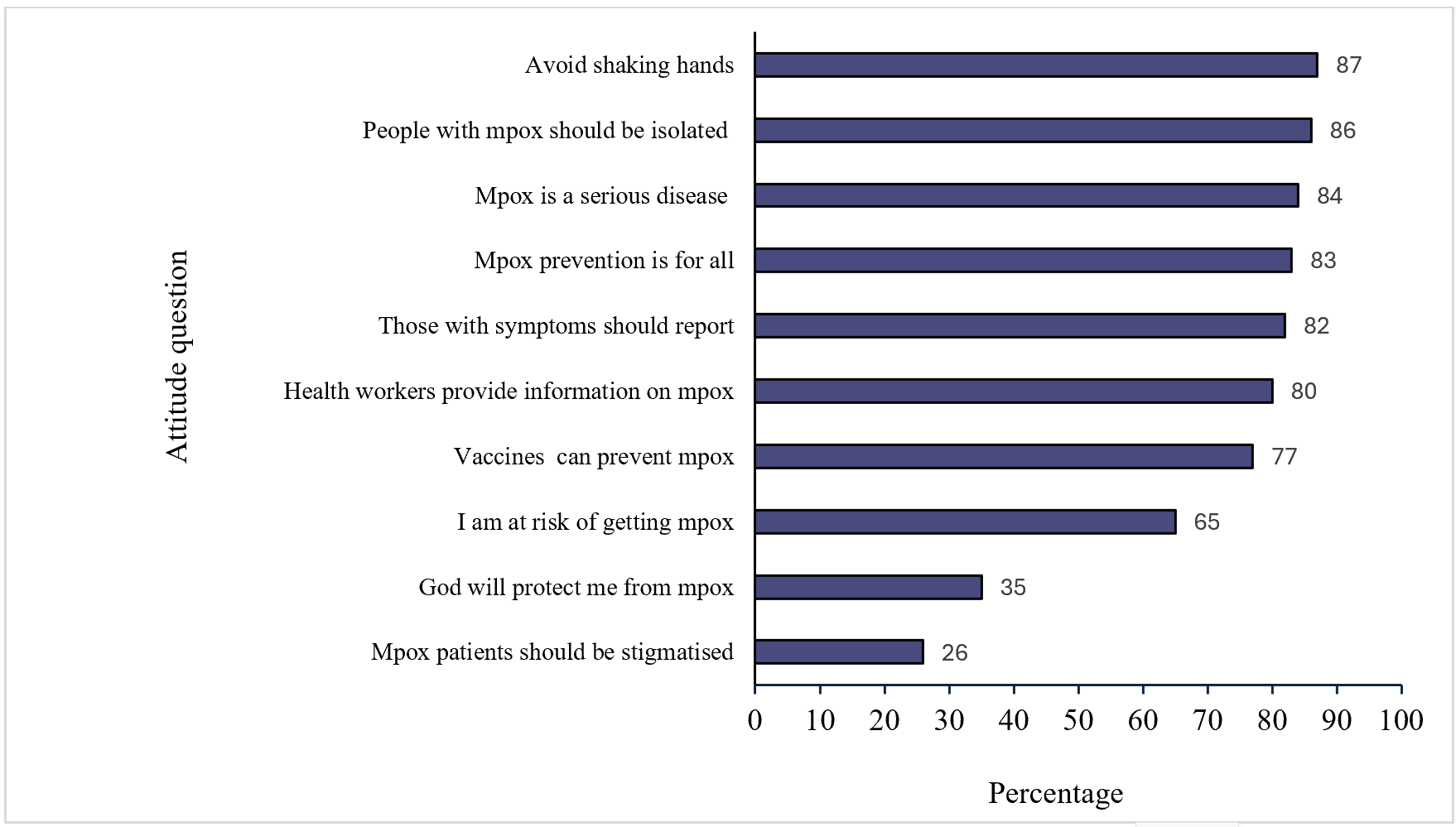
Overall, attitudes towards mpox prevention were favourable, with 1,252 (87%) willing to adopt preventive behaviours, including avoiding handshakes and supporting isolation of persons with mpox-like symptoms, 1,237(86%). A high proportion, 1,209 (84%), perceived mpox as a serious disease and agreed that prevention requires collective action, 1,194 (83%). In addition, 1,179 (82%) supported prompt reporting of symptoms, and 1,150 (80%) valued information provided by health workers. Vaccine acceptance was moderate, with 1,108 (77%) acknowledging that vaccination can prevent mpox. Risk perception varied: 935 (65%) perceived themselves as at risk during the gathering, whereas 503 (35%) expressed reliance on divine protection. Stigmatizing attitudes were reported by 374 (26%) of participants (Figure 2).
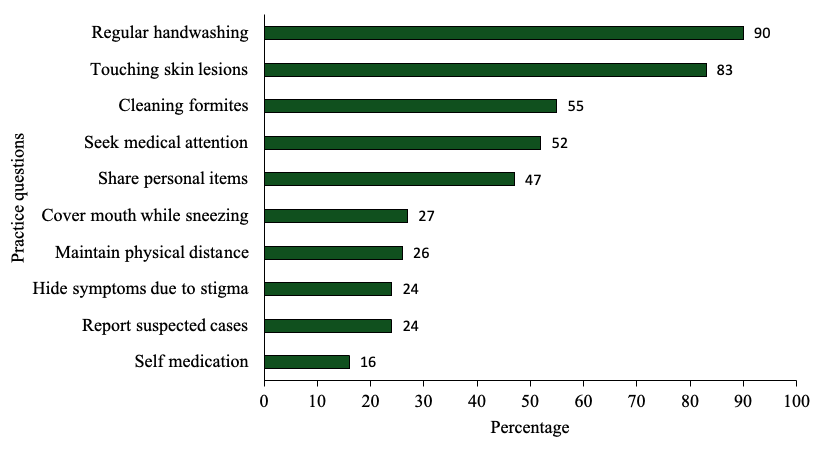
Preventive practices were mixed. Most participants (1,294; 90%) reported regular handwashing, and 1,194 (83%) reported avoiding direct contact with skin lesions. Cleaning of potentially contaminated surfaces and seeking medical care were reported by approximately half of the participants. However, several key preventive behaviours were less common, including maintaining physical distance (374; 26%), covering the mouth when sneezing (388; 27%), and reporting suspected cases (345; 24%). Nearly half reported sharing personal items (676, 47%), and 230 (16%) reported self-medication. Overall, only 345 (24%) met the criteria for good preventive practices (Figure 3).
Factors associated with knowledge, attitudes, and practices
In multivariable analysis, adequate knowledge of mpox was associated with increasing age and higher educational attainment. Compared with participants aged 18–29 years, those aged 45–59 years were more than twice as likely to have adequate knowledge adjusted prevalence ratio (aPR=2.40; 95%CI:1.80–3.10), whereas no significant difference was observed among those aged ≥60 years (aPR=1.00; 95%CI:0.85–1.18).
Education demonstrated a strong dose–response relationship. Compared with participants with no formal education, those with primary (aPR=2.70; 95%CI:1.90–3.90), secondary (aPR=6.10; 95%CI: 4.50–8.20), and tertiary education (aPR=7.20; 95% CI: 5.20–9.80) were progressively more likely to have adequate knowledge. Male participants had slightly higher knowledge than female participants (aPR=1.10; 95% CI: 1.02–1.20) (Table 2).
Positive attitudes towards mpox prevention were associated with age and education. Compared with participants aged 18–29 years, those aged 30–44 years were more likely to report a positive attitude (aPR=1.90; 95%CI:1.30–2.70), whereas no significant differences were observed among older age groups.
Higher educational attainment was strongly associated with positive attitudes. Compared with participants with no formal education, those with primary (aPR=2.20; 95% CI:1.30–3.80), secondary (aPR=4.90;95% CI:2.70–8.90), and tertiary education (aPR=6.10; 95% CI: 3.30–11.10) were more likely to have positive attitudes (Table 3).
Good preventive practices were low across all sociodemographic groups. In both bivariate and multivariable analyses, no participant characteristics were significantly associated with good practices (Table 4). Mpox prevention practices were low across all sociodemographic groups. In bivariate analysis, no factors were associated with good preventive practices and the same applied during multivariable analysis (Table 4).
In this cross-sectional assessment conducted during a large national mass gathering in Uganda, awareness of mpox was high and attitudes towards prevention were generally favourable; however, adoption of preventive practices was limited. Knowledge and attitudes were associated with age and level of education, whereas no sociodemographic factors were associated with preventive practices. These findings highlight a gap between awareness and behaviour in a high-risk setting characterized by close contact and population mixing.
The high level of awareness is likely attributable to intensified risk communication and community engagement efforts by the Ministry of Health, alongside media coverage during a period of heightened outbreak preparedness [11]. Similar findings have been reported in both endemic and non-endemic settings during recent mpox outbreaks [12, 13]. Despite high awareness, knowledge gaps persisted, particularly regarding vaccination as a preventive strategy and the increased risk among people living with HIV.
Comparable findings have been documented in studies from Nigeria, Ghana, and Europe [14, 15]. These observations suggest that public health messaging may prioritize disease recognition and severity while placing less emphasis on preventive measures and less intuitive transmission pathways.
Attitudes towards mpox prevention were generally favourable, including support for isolation, reporting of symptoms, and reliance on healthcare worker guidance. This likely reflects heightened perceived risk during an active outbreak [16, 17]. However, the persistence of beliefs in divine protection highlights the influence of cultural and religious contexts on health behaviour in pilgrimage settings and underscores the importance of engaging faith-based structures in risk communication efforts.
Preventive practices were inconsistent. Basic hygiene behaviours were widely adopted, but practices that disrupt social interaction or pilgrimage routines, such as physical distancing, avoiding sharing personal items, and reporting symptoms, were implemented less consistently. These patterns likely reflect structural and contextual constraints inherent to mass gatherings, including overcrowding, limited personal space, shared accommodation, stigma and concerns about isolation. [15]. Similar gaps between knowledge, attitudes, and practices have been documented in studies on mpox and other infectious diseases, indicating that awareness and favourable attitudes do not necessarily translate into sustained behaviour change [12, 18, 19].
Educational attainment and age were important determinants of knowledge and attitudes. Higher education was associated with improved knowledge and more favourable attitudes, consistent with evidence that education enhances access to, interpretation of, and health information [20, 21]. Older participants also demonstrated greater knowledge, possibly reflecting cumulative exposure to prior outbreaks and increased perceived vulnerability [22]. These findings highlight the need for targeted communication strategies that address the information needs and media consumption patterns of younger populations.
The absence of associations between individual characteristics and preventive practices suggests that behaviour in this setting is shaped primarily by environmental and contextual factors rather than by knowledge alone. Although not directly measured, crowd density, shared accommodation, and limited WASH infrastructure likely constrained adherence to recommended measures. This interpretation is consistent with the socioecological model, which emphasizes the influence of structural conditions on individual behaviour [23-25]. Interventions should therefore combine targeted health education with context-appropriate measures that enable individuals to adopt recommended practices in high-density environments [26, 27]. These findings have important implications for outbreak preparedness and response in mass gatherings. Risk communication strategies should focus not only on increasing awareness but also on addressing practical and social barriers to behaviour change. Structural interventions, including improving access to hand hygiene facilities, enhancing crowd management, and establishing accessible systems for symptom reporting, are critical to support the adoption of preventive practices. Integrating community and faith leaders into response efforts may further improve the acceptability and uptake of interventions.
Study limitations
This assessment has several limitations. First, data were self-reported and may be subject to social desirability bias, with participants potentially overstating knowledge or adherence to recommended practices. Second, the cross-sectional design captures a single time point and does not allow assessment of changes in knowledge, attitudes, or practices over time. Third, although participants were drawn from across the country, the findings are based on a mass gathering context and may not fully represent behaviours in other community settings. Finally, the systematic intercept sampling approach may limit generalizability due to potential selection bias.
Knowledge and attitudes towards mpox were moderate, but adoption of preventive practices remained low. Knowledge and attitudes were associated with age and educational attainment, highlighting disparities in access and interpretation of health information. The observed gap between awareness and behaviour suggests that awareness alone may be insufficient to change behaviour. Future public health responses should combine targeted and culturally sensitive risk communication with practical enabling interventions, including the deployment of temporary hand hygiene stations, accessible symptom reporting and referral systems, multilingual health messaging, improved crowd management, and the engagement of community and religious leaders. Integrating these measures into mass gathering preparedness and response plans could enhance adherence to preventive behaviours and strengthen outbreak prevention and control efforts.
What is already known about the topic
What this study adds
The authors of this work declare no competing interests.
Data availability
The datasets generated and analysed during this study are the property of the Uganda Public Health Fellowship Program and are not publicly available to protect participant confidentiality. However, data can be made available from the corresponding author upon reasonable request, subject to approval by the Uganda Public Health Fellowship Program.
This study was supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the US Centres for Disease Control and Prevention (CDC) under Cooperative Agreement number GH001353-01, awarded to Makerere University School of Public Health for the Uganda Public Health Fellowship Program, Ministry of Health.
Disclaimer
The findings and conclusions presented in this report are those of the authors and do not necessarily reflect the official views of the US Centres for Disease Control and Prevention, the Department of Health and Human Services, Makerere University School of Public Health, or the Uganda Ministry of Health.
We acknowledge the Ministry of Health and the Uganda Public Health Fellowship Program for their technical guidance. We also thank the Department of Integrated Epidemiology and Public Health Emergencies for spearheading this activity. In addition, we appreciate Master of Public Health students from Makerere University, School of Public Health, who assisted us with data collection.
MDN, AN, JW, RM, BK, DK, BL, EO, and ARA contributed to this work. MDN led study conception, field coordination, data analysis, and manuscript drafting. AN, JW, and RM supported the study design, tool development, oversight of data collection, and interpretation of results. BK, BL, RM and ARA provided senior technical guidance, methodological validation, and critical review of the manuscript. DK and EO supported data management, analysis, and interpretation. All authors reviewed and approved the final manuscript.
| Variable | Frequency (n=1,438) | Percentage (%) |
|---|---|---|
| Age (years) | ||
| 18–29 | 575 | 40 |
| 30–44 | 560 | 39 |
| 45–59 | 213 | 15 |
| ≥60 | 90 | 6 |
| Sex | ||
| Female | 614 | 43 |
| Male | 824 | 57 |
| Marital status | ||
| Married | 621 | 43 |
| Separated | 42 | 3 |
| Single | 600 | 42 |
| Widow(er) | 193 | 13 |
| Level of education | ||
| None | 79 | 5 |
| Primary | 463 | 32 |
| Secondary | 638 | 44 |
| Tertiary | 258 | 18 |
| Occupation | ||
| Business | 832 | 58 |
| Formal employment | 244 | 17 |
| None | 325 | 23 |
| Casual laborer | 37 | 2 |
| Region | ||
| Central | 659 | 46 |
| Eastern | 306 | 21 |
| Northern | 93 | 6 |
| Western | 380 | 26 |
| Variable | Knowledge | cPR (95% CI) | aPR (95% CI) | |
|---|---|---|---|---|
| Good n (%) n=575 | Poor n (%) n=863 | |||
| Age (years) | ||||
| 18–29 | 210 (37) | 365 (63) | Ref | Ref |
| 30–44 | 250 (45) | 310 (55) | 1.22 (1.10–1.35) | 1.10 (1.02–1.15) |
| 45–59 | 180 (85) | 33 (15) | 2.32 (2.10–2.56) | 2.40 (1.80–3.10) |
| ≥60 | 36 (40) | 54 (60) | 1.10 (0.90–1.34) | 1.00 (0.85–1.18) |
| Sex | ||||
| Female | 230 (38) | 384 (62) | Ref | Ref |
| Male | 340 (41) | 484 (59) | 1.10 (1.01–1.21) | 1.10 (1.02–1.20) |
| Education | ||||
| None | 10 (13) | 69 (87) | Ref | Ref |
| Primary | 122 (26) | 341 (74) | 2.08 (1.20–3.60) | 2.70 (1.90–3.90) |
| Secondary | 180 (28) | 458 (72) | 2.22 (1.30–3.80) | 6.10 (4.50–8.20) |
| Tertiary | 65 (25) | 193 (75) | 1.98 (1.10–3.50) | 7.20 (5.20–9.80) |
| Ref: Reference; cPR: crude Prevalence Ratio; aPR: adjusted Prevalence Ratio; CI: confidence interval | ||||
| Variable | Attitude | cPR (95% CI) | aPR (95% CI) | |
|---|---|---|---|---|
| Yes (n, %) n=576 | No (n, %) n=862 | |||
| Age (years) | ||||
| 18–29 | 172 (30) | 403 (70) | Ref | Ref |
| 30–44 | 319 (57) | 241 (43) | 1.91 (1.65–2.20) | 1.90 (1.30–2.70) |
| 45–59 | 64 (30) | 149 (70) | 1.00 (0.79–1.28) | 1.00 (0.60–1.60) |
| ≥60 | 24 (27) | 66 (73) | 0.89 (0.62–1.29) | 0.90 (0.50–1.50) |
| Sex | ||||
| Female | 246 (40) | 368 (60) | Ref | Ref |
| Male | 330 (40) | 494 (60) | 1.00 (0.88–1.13) | 1.00 (0.80–1.20) |
| Education | ||||
| None | 16 (20) | 63 (80) | Ref | Ref |
| Primary | 204 (44) | 259 (56) | 2.17 (1.39–3.40) | 2.20 (1.30–3.80) |
| Secondary | 447 (70) | 191 (30) | 3.45 (2.22–5.37) | 4.90 (2.70–8.90) |
| Tertiary | 206 (80) | 52 (20) | 3.93 (2.53–6.11) | 6.10 (3.30–11.10) |
| Ref: Reference; cPR: crude Prevalence Ratio; aPR: adjusted Prevalence Ratio; CI: confidence interval | ||||
| Variable | Practices | cPR (95% CI) | aPR (95% CI) | |
|---|---|---|---|---|
| Good (n, %) n=345 |
Poor (n, %) n=1,093 |
|||
| Age (years) | ||||
| 18–29 | 130 (23) | 445 (77) | Ref | Ref |
| 30–44 | 150 (27) | 410 (73) | 1.17 (0.93–1.47) | 1.15 (0.85–1.55) |
| 45–59 | 45 (21) | 168 (79) | 0.91 (0.66–1.27) | 0.90 (0.60–1.30) |
| ≥60 | 20 (22) | 70 (78) | 0.96 (0.61–1.51) | 0.95 (0.55–1.60) |
| Sex | ||||
| Female | 150 (24) | 464 (76) | Ref | Ref |
| Male | 195 (24) | 629 (76) | 1.00 (0.82–1.22) | 1.00 (0.75–1.30) |
| Education level | ||||
| None | 12 (15) | 67 (85) | Ref | Ref |
| Primary | 100 (22) | 363 (78) | 1.47 (0.83–2.60) | 1.40 (0.70–2.80) |
| Secondary | 170 (27) | 468 (73) | 1.80 (1.02–3.20) | 1.70 (0.90–3.20) |
| Tertiary | 63 (24) | 195 (76) | 1.60 (0.88–2.90) | 1.50 (0.70–3.10) |
| Ref: Reference; cPR: crude Prevalence Ratio; aPR: adjusted Prevalence Ratio; CI: confidence interval | ||||