Lessons from the field | Open Access | Volume 9 (2): Article 99 | Published: 16 Jun 2026
Views: 57
Menu, Tables and Figures
| No | Period | Activity / project title | Project type or data source | Response function(s) | Output used for synthesis |
|---|---|---|---|---|---|
| 1 | July-August 2024 | Investigation of the first confirmed Mpox outbreak in Kasese District, western Uganda | Outbreak investigation report; descriptive field investigation | Epidemiologic investigation; surveillance and case detection | Completed outbreak investigation report; manuscript under review |
| 2 | July-October 2024 | Factors associated with Mpox severity in Uganda (MPSSS validation) | Analytic epidemiologic study using national Mpox case data | Clinical severity, outcomes, and care models | Completed analytic study; manuscript in preparation; public health bulletin article[15] |
| 3 | July-December 2024 | Delayed patient isolation and associated factors during the Mpox outbreak in Uganda | Analytic epidemiologic study using case investigation and isolation data | Surveillance and case detection; RCCE | Completed analytic study report; manuscript published [4] |
| 4 | July 2024-February 2025 | Evaluation of performance and impact of contact tracing during the Mpox outbreak in Uganda | National program evaluation using contact tracing records | Surveillance and case detection; health system and workforce capacity | Completed national evaluation report; manuscript in preparation |
| 5 | July 2024-February 2025 | Risk factors for Mpox transmission among household contacts in Uganda | Analytic epidemiologic study among household contacts | Epidemiologic investigation and transmission dynamics | Completed analytic study; manuscript in preparation |
| 6 | August-September 2024 | Epidemiological profile of early Mpox cases in Uganda | Descriptive analysis of early national case data | Surveillance and case detection; epidemiologic investigation | Completed descriptive epidemiologic analysis; manuscript under review |
| 7 | August-September 2024 | Assessment of healthcare workers knowledge, attitudes, and practices toward Mpox in Uganda | Cross-sectional KAP study among healthcare workers | Risk communication and community engagement; workforce readiness | Completed analytic report; manuscript under review; public health bulletin article [16] |
| 8 | August-October 2024 | Psychological distress and perceived Mpox risk among healthcare workers during early outbreak phase | Cross-sectional psychosocial assessment among healthcare workers | Psychosocial impact and stigma; healthcare worker wellbeing | Completed analytic report; manuscript under review |
| 9 | August-September 2024 | Mpox outbreak investigation in fishing communities of Nakasongola District | Outbreak investigation report; descriptive field investigation | Epidemiologic investigation and transmission dynamics | Completed outbreak investigation report; manuscript in preparation; public health bulletin article [12] |
| 10 | August 2024-January 2025 | Epidemiology, clinical features, and outcomes of Mpox in children and adolescents in Uganda | Analytic study of pediatric and adolescent case data | Clinical severity, outcomes, and care models | Completed analytic study; manuscript published [3] |
| 11 | August 2024-January 2025 | Stigma and associated factors among Mpox survivors in Kampala Metropolitan Area | Cross-sectional study among Mpox survivors | Psychosocial impact and stigma | Completed analytic study; public health bulletin article; manuscript published [19] |
| 12 | August 2024-May 2025 | Factors associated with Mpox-related mortality in Uganda | Analytic epidemiologic study using national case outcome data | Clinical severity, outcomes, and care models | Completed analytic study; manuscript in preparation |
| 13 | September-October 2024 | Coordinated outbreak investigations in Mityana and Namayingo Districts | Coordinated district outbreak investigation reports | Epidemiologic investigation and transmission dynamics | Completed investigation reports; programmatic outputs |
| 14 | September-October 2024 | Investigation of Mpox outbreak in Mityana District, Uganda | District outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 15 | September-October 2024 | Mpox outbreak investigation in Namayingo District | District outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 16 | October 2024 | Mpox outbreak investigation in prison settings (Masindi Prison) | Institutional outbreak investigation report | Epidemiologic investigation and transmission dynamics; health system capacity | Completed outbreak investigation report; public health bulletin article [13] |
| 17 | October 2024-January 2025 | Evaluation of alert management system during Mpox response in Kampala Metropolitan Area | Surveillance system evaluation using alert management records | Surveillance and case detection | Completed evaluation report; manuscript in preparation |
| 18 | October 2024-March 2025 | Mpox outbreak investigation in Mbarara City, Uganda | City outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed outbreak investigation report; public health bulletin article [39] |
| 19 | October 2024-May 2025 | Mpox outbreak investigation in Greater Mbarara (urban and peri-urban settings) | Analytic synthesis of outbreak investigation data | Epidemiologic investigation and transmission dynamics | Completed analytic synthesis; manuscript under review[20] |
| 20 | October 2024-May 2025 | Laboratory rapid response assessment and intervention during the Mpox outbreak in Greater Mbarara, Uganda | Laboratory rapid response assessment and intervention documentation | Laboratory-epidemiology interface | Laboratory assessment and intervention report; programmatic output |
| 21 | October 2024-May 2025 | Factors associated with Mpox misdiagnosis in Mbarara City | Analytic epidemiologic study using clinical encounter data | Laboratory-epidemiology interface; surveillance and case detection | Completed analytic study; public health bulletin article[40] |
| 22 | October 2024-April 2025 | Predictors of time to recovery among Mpox patients admitted at Mbarara Regional Referral Hospital | Analytic study among hospitalized Mpox patients | Clinical severity, outcomes, and care models | Completed analytic study; manuscript in preparation |
| 23 | October-November 2024 | Mpox case investigations in Kampala Metropolitan Area (Mukono, Wakiso, Kampala) | Case investigation reports across Kampala Metropolitan Area | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 24 | November 2024 | Mpox outbreak investigation at Sowe Island, Mukono District | Island outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed outbreak investigation report; public health bulletin article [14] |
| 25 | December 2024 | Individual and household factors of Mpox among household contacts in Nakasongola and Mayuge Districts | Analytic report among household contacts | Epidemiologic investigation and transmission dynamics; RCCE | Completed analytic report; programmatic output |
| 26 | January-February 2025 | Resilience and associated factors among healthcare workers in Mpox treatment units | Cross-sectional assessment among healthcare workers | Psychosocial impact and stigma; workforce wellbeing | Completed analytic study; manuscript under peer review |
| 27 | January-February 2025 | Post-traumatic stress disorder, depression, and anxiety among Mpox survivors in central Uganda | Cross-sectional psychosocial assessment among survivors | Psychosocial impact and stigma | Completed analytic study; manuscript in preparation |
| 28 | February 2025 | Knowledge, attitudes, and practices of community health workers regarding Mpox in Mbarara City | Cross-sectional KAP study among community health workers | Risk communication and community engagement | Completed analytic study; manuscript published [41] |
| 29 | February 2025 | Prevalence and determinants of Mpox vaccine acceptance among healthcare workers in Kampala Metropolitan Area | Cross-sectional study among healthcare workers | Risk communication and community engagement | Completed analytic study report; public health bulletin article [18] |
| 30 | February-March 2025 | Enhancing capacity for Mpox surveillance through mentorship in high-risk districts | Mentorship and training reports | Health system and workforce capacity; surveillance and case detection | Mentorship reports; training of approximately 160 health workers |
| 31 | March 2025 | Epidemiological investigation of Mpox outbreak on Lyabana Island, Buvuma District | Island outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 32 | April 2025 | Mpox outbreak investigation in Kiryandongo District and Hoima City | District and city outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 33 | May 2025 | Factors associated with delayed care-seeking among Mpox cases in Mbarara City | Analytic epidemiologic study using case investigation data | Clinical severity, outcomes, and care models; RCCE | Completed analytic study; manuscript under development |
| 34 | May 2025 | Prevalence and factors associated with Mpox severity in Nyamityobora ward, Mbarara City | Analytic study using ward-level case data | Clinical severity, outcomes, and care models | Completed analytic study; manuscript in preparation |
| 35 | June 2025 | Knowledge, attitudes, and practices on Mpox among pilgrims during Martyrs Day commemoration | Cross-sectional KAP assessment among pilgrims | Risk communication and community engagement | Completed analytic report; manuscript in preparation |
| 36 | 2024-2025 | Development of a real-time Mpox surveillance dashboard in collaboration with the United States CDC | Operational dashboard development and surveillance data integration | Surveillance and case detection; laboratory-epidemiology interface | Operational dashboard implemented |
Note. Response functions are not mutually exclusive; a project could contribute to more than one response function where applicable. Output status refers to outputs available for this synthesis at the time of manuscript preparation; unpublished reports are programmatic response outputs, not peer-reviewed publications.
Table 1: Mpox-related response activities undertaken by Uganda Public Health Fellowship Program fellows, Uganda, 2024-2025
| Response function / operational focus | Project outputs contributing to this domain | Descriptive findings from project outputs | Response relevance or recommendations from project outputs |
|---|---|---|---|
| Under-reporting and misdiagnosis | Misdiagnosis study in Mbarara City; delayed isolation analysis; surveillance reviews | Project outputs documented delayed recognition and frequent initial alternative diagnoses, especially in private facilities. | Supported recommendations for targeted orientation of private facilities, dissemination of case definitions, and Mpox screening in outpatient settings. |
| Alert management and surveillance performance | Kampala Metropolitan Area alert-management evaluation; surveillance data quality reviews | Project outputs documented alert triage, documentation, and timeliness gaps. | Supported recommendations for improving alert documentation, triage procedures, and routine data quality review. |
| Laboratory-epidemiology coordination and diagnostic response | Greater Mbarara laboratory rapid response assessment; dashboard development; diagnostic-delay related studies | Project outputs documented sample transport, turnaround time, and coordination constraints between surveillance and laboratory teams. | Supported recommendations to improve specimen referral, laboratory turnaround time monitoring, and integration of laboratory and epidemiologic data. |
| Early transmission dynamics | District outbreak investigations in Kasese, Nakasongola, Mbarara, KMA, Mukono, Masindi Prison, Mityana, Namayingo, Buvuma, Hoima, and Kiryandongo | Project outputs described transmission patterns across urban, fishing, island, institutional, and community settings. | Supported geographic prioritization of response activities and population-specific risk communication. |
| Household and non-sexual transmission | Household-contact analyses; home-based-care related assessments | Project outputs documented transmission in household settings and potential exposure through close contact and shared items. | Supported recommendations to extend messaging beyond sexual networks to households, caregivers, and home-based care settings. |
| Pediatric Mpox | Analysis of children and adolescents with Mpox | Project outputs described clinical features and outcomes among children and adolescents. | Supported recommendations for pediatric-focused clinical guidance and school/community messaging. |
| Delayed care-seeking and isolation | Delayed isolation analysis; delayed care-seeking analysis in Mbarara City | Project outputs documented delayed care-seeking, delayed isolation, and barriers including self-medication, low perceived risk, and access constraints. | Supported recommendations for early-care-seeking messages and frontline diagnostic orientation. |
| Clinical severity, mortality, recovery, and care models | Severity analysis; mortality analysis; recovery-time analysis; home-based and facility-based care evaluations | Project outputs described patterns of severity, mortality, recovery, and care model implementation. | Supported recommendations for risk stratification, referral prioritization, and context-specific case management planning. |
| Contact tracing implementation | National contact tracing evaluation | Project outputs documented initiation, follow-up, completion, and implementation constraints in contact tracing. | Supported recommendations to refine contact tracing procedures and align resources with feasible response strategies. |
| Health system and workforce capacity | Mentorship and training reports; health system assessments; PPE, isolation, and operational support reviews | Project outputs documented workforce training coverage and operational constraints affecting response activities. | Supported recommendations for emergency logistics, training, supervision, and workforce support. |
| Risk communication and community engagement | KAP studies among health workers, community health workers, pilgrims, and affected communities; vaccine acceptance study | Project outputs documented gaps in knowledge, reporting, referral, prevention practices, and vaccine concerns. | Supported recommendations for targeted RCCE messages for health workers, community health workers, mobile populations, caregivers, and communities. |
| Psychosocial impact, stigma, and survivor wellbeing | Stigma study among survivors; PTSD, depression, and anxiety study; healthcare worker psychosocial assessments | Project outputs documented stigma, mental health symptoms, and psychosocial concerns among survivors and healthcare workers. | Supported recommendations to integrate psychosocial support and stigma reduction into Mpox care and response pathways. |
| Healthcare worker resilience and occupational wellbeing | Resilience study among healthcare workers in Mpox treatment units; psychological distress assessment | Project outputs documented occupational stressors, perceived risk, and resilience-related concerns among frontline workers. | Supported recommendations for infection prevention support, staff wellbeing interventions, and resilience-oriented supervision. |
RCCE, risk communication and community engagement; PPE, personal protective equipment; KMA, Kampala Metropolitan Area; PTSD, post-traumatic stress disorder.
Table 2: Operational contributions of Mpox response projects conducted by Uganda Public Health Fellowship Program fellows, Uganda, 2024-2025
Richard Migisha1,&, Benon Kwesiga1, Samuel Gidudu1, Lilian Bulage1, Ivan Lukabwe1, Alex Riolexus Ario1
1Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda
&Corresponding author: Richard Migisha, Uganda Public Health Fellowship Program, Uganda National Institute of Public Health, Kampala, Uganda, Email: rmigisha@uniph.go.ug ORCID: https://orcid.org/0000-0003-1709-9521
Received: 10 Mar 2026, Accepted: 10 Jun 2026, Published: 16 Jun 2026
Domain: Field Epidemiology
Keywords: Mpox, Disease Outbreaks, Field Epidemiology, Public Health Surveillance, Health Workforce, Laboratory Services, Risk Communication, Uganda
©Richard Migisha et al. Journal of Interventional Epidemiology and Public Health (ISSN: 2664-2824). This is an Open Access article distributed under the terms of the Creative Commons Attribution International 4.0 License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cite this article: Richard Migisha et al., Contributions of the Uganda Public Health Fellowship Program to the 2024–2025 mpox response. Journal of Interventional Epidemiology and Public Health. 2026; 9(02):99. https://doi.org/10.37432/jieph-d-26-00076
Introduction: Uganda experienced a protracted Mpox outbreak during 2024–2025, with cases reported across 100 of 146 districts by late April 2025. Fellows from the Uganda Public Health Fellowship Program (UPHFP), drawn from the Field Epidemiology Training Program (Advanced FETP) and the Laboratory Leadership Program (LLP), were deployed within national and subnational response structures to support surveillance, laboratory coordination, outbreak investigation, and analytic activities. We describe the contributions of these programs to Uganda’s Mpox response.
Methods: We conducted a descriptive programmatic review of Mpox-related response activities implemented by UPHFP fellows during July 2024–June 2025. Data sources included outbreak investigation reports, analytic studies, and mentorship reports. Projects were synthesised using nationally adapted WHO response pillars.
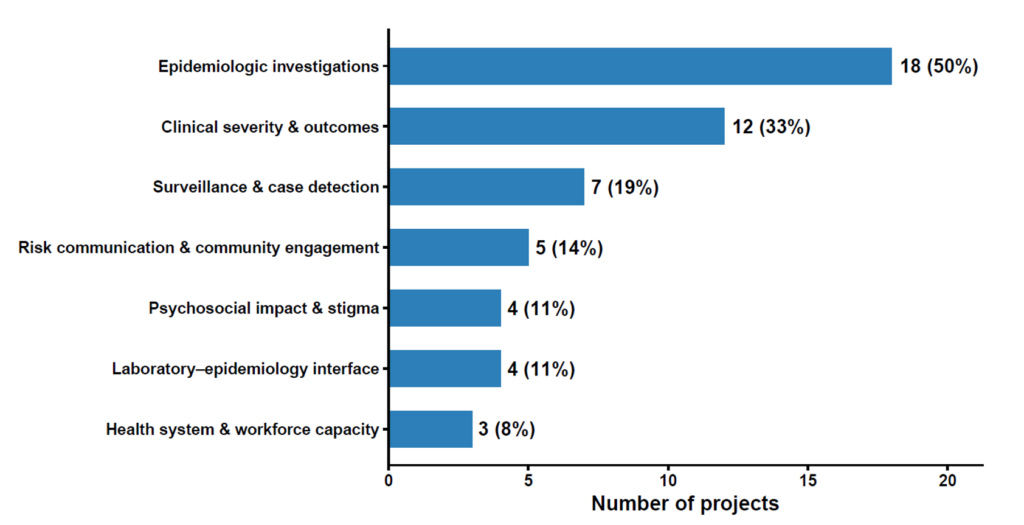
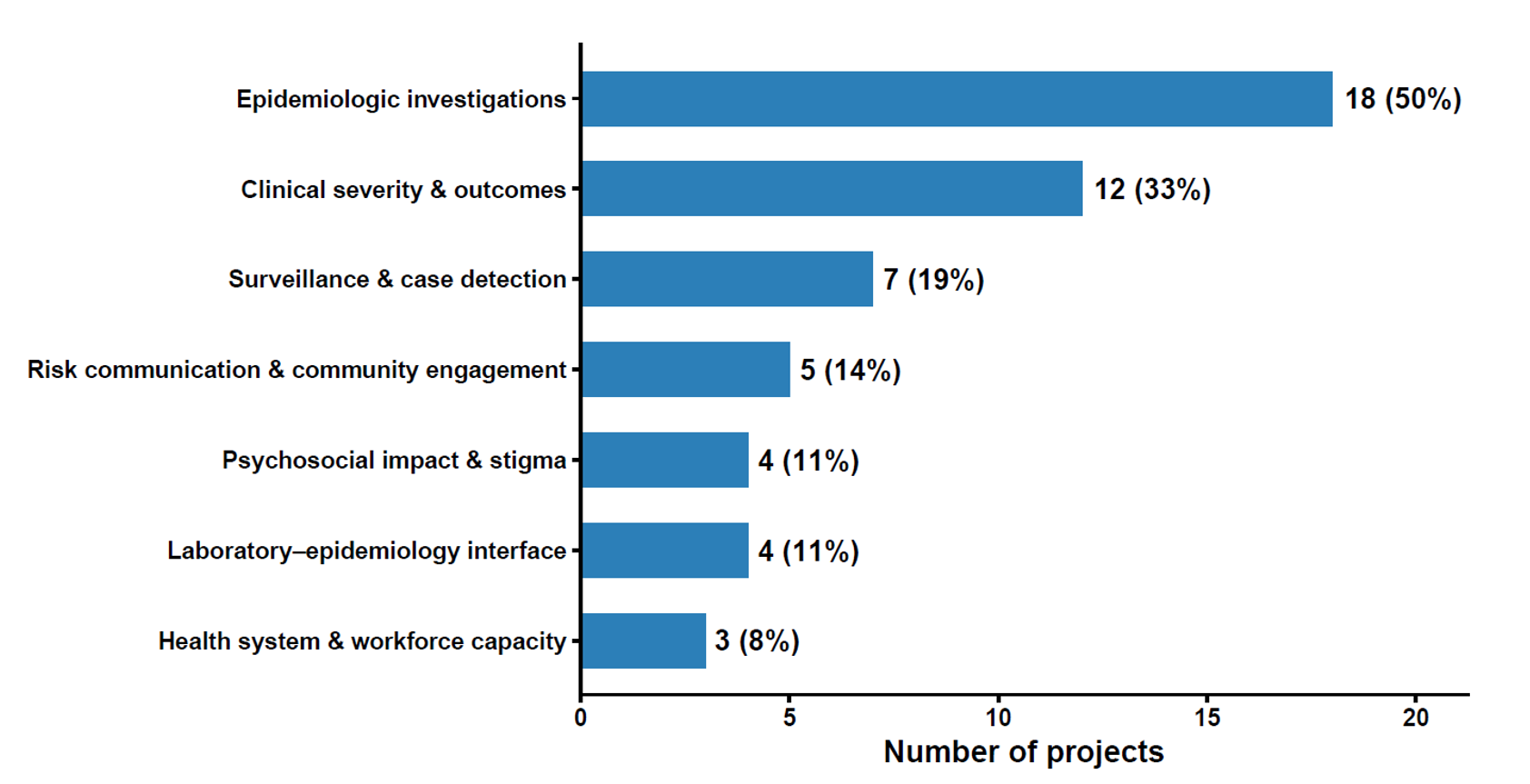
Results: Fellows conducted 36 mpox-related projects across urban, peri-urban, island, fishing-community, institutional, healthcare, and household settings. Projects contributed to epidemiologic investigations and transmission dynamics (18/36, 50%), clinical severity and outcomes (12/36; 33%), surveillance and case detection (7/36; 19%), risk communication and community engagement (5/36; 14%), laboratory–epidemiology coordination (4/36; 11%), psychosocial impact and stigma (4/36; 11%), and health system and workforce capacity (3/36; 8%). Outputs included reports, analytic studies, dashboards, laboratory assessments, and mentorship reaching approximately 160 health workers across 30 districts. Project outputs documented delayed diagnosis, under-reporting, household transmission, severity patterns, health system constraints, and psychosocial effects among survivors and healthcare workers.
Conclusion: UPHFP fellows contributed broad operational and analytic support to Uganda’s mpox response. Embedding field epidemiology and laboratory leadership fellows within response structures can support evidence-informed outbreak response and preparedness.
Mpox, historically endemic in parts of Africa, re-emerged as a global threat during the 2022 multi-country outbreaks, demonstrating both its epidemic potential and the importance of coordinated public health response measures [1]. The subsequent emergence of clade Ib in late 2023 led to renewed regional spread in Central and East Africa, including Uganda, where the outbreak was first confirmed in late July 2024 in Kasese District, western Uganda[1]. The outbreak rapidly expanded beyond the initial affected area; by late April 2025, Uganda had reported 5,725 confirmed Mpox cases and 40 deaths across 100 of 146 districts, reflecting sustained nationwide transmission and substantial response demands[2]. Disease severity and transmission patterns varied widely across settings, including urban centres, fishing communities, island districts, prisons, and schools, placing heavy demands on surveillance, outbreak investigations, and response coordination[3-5].
Effective outbreak control, including mpox, relies not only on medical countermeasures but also on a skilled workforce, such as field epidemiologists capable of rapidly detecting cases, characterising transmission, identifying high-risk populations, and translating findings into response actions [6]. Field Epidemiology Training Programs have been established in many countries to build this capacity through competency-based, service-oriented training that combines classroom instruction with mentored field practice [7]. In Uganda, the Uganda Public Health Fellowship Program (UPHFP) is implemented through the Uganda National Institute of Public Health under the Ministry of Health and includes several tracks, including the Advanced Field Epidemiology Training Program (Advanced FETP) and the Laboratory Leadership Program (LLP) [8]. These two tracks were central to the Mpox response because Advanced FETP fellows supported surveillance, outbreak investigation, and epidemiologic analysis, while LLP fellows strengthened laboratory leadership, diagnostic coordination, and the laboratory–epidemiology interface.
Although individual mpox investigations and analytic studies conducted during the response generated important operational findings, their collective contribution to Uganda’s national response has not been systematically described. This gap is important because outbreak responses often depend on multiple concurrent activities—surveillance evaluations, field investigations, laboratory assessments, clinical analyses, risk communication studies, workforce mentorship, and psychosocial assessments—that are rarely synthesised as a portfolio of workforce contributions[9, 10]. Documenting these contributions can clarify how embedded field epidemiology and laboratory leadership fellows supported response functions across different phases of the epidemic and can inform future investments in outbreak workforce capacity. We therefore conducted a descriptive programmatic review to synthesise mpox-related response activities undertaken by Advanced FETP and LLP fellows under the Uganda Public Health Fellowship Program between July 2024 and June 2025. Specifically, we aimed to describe the scope, geographic distribution, response functions, and operational contributions of fellows’ projects to Uganda’s 2024–2025 mpox response.
Study design, scope and setting
We conducted a descriptive, programmatic review of mpox response activities undertaken by Advanced FETP and LLP fellows in Uganda between July 2024 and June 2025. UPHFP is a two-year, competency-based training program implemented by the Uganda Ministry of Health through the UNIPH, with technical and financial support from the Centres for Disease Control and Prevention. The programs aim to strengthen Uganda’s public health workforce by combining classroom instruction with mentored, field-based service during real-world public health responses. UPHFP is implemented across 6 tracks: Field Epidemiology, Laboratory Leadership, Health Informatics, Prevention Effectiveness, Implementation Science, and Monitoring and Evaluation [8]. This review focused on the Advanced FETP and LLP tracks because these were the UPHFP tracks directly engaged in the field epidemiology, outbreak investigation, analytic epidemiology, laboratory leadership, and laboratory-epidemiology coordination activities captured in the mpox response documentation. During the 2024-2025 mpox response, fellows from these tracks were embedded within national and subnational response structures, including Ministry of Health response teams, district response teams, surveillance structures, laboratory coordination platforms, and partner-supported response activities.
Data sources
Data were derived from routine outputs generated as part of the national mpox response, including: outbreak investigation reports at district, regional, and national levels; surveillance system and alert management evaluations; analytic epidemiologic studies examining risk factors, clinical severity, mortality, and recovery; health system and workforce assessments; community, behavioural, and mental health studies; and documentation of mentorship and capacity-building activities. Analytic studies included project-specific cross-sectional, case-control, cohort, and descriptive epidemiologic analyses conducted as part of the response. These source materials were produced under the leadership or co-leadership of UPHFP fellows in collaboration with the Uganda Ministry of Health, UNIPH, district health teams, laboratories, and implementing partners.
Identification and inclusion of projects
Mpox-related projects were eligible for inclusion if they were implemented during the July 2024 to June 2025 response period, involved Advanced FETP or LLP fellows as lead investigators or major technical contributors, and generated outputs relevant to outbreak detection, investigation, response coordination, laboratory-epidemiology coordination, clinical or epidemiologic characterisation, health system strengthening, community engagement, workforce capacity, or psychosocial support. Projects that were not related to the mpox response, did not involve fellows from the selected UPHFP tracks, or did not generate a documented programmatic or analytic output were excluded.
Data abstraction
Each eligible project was reviewed using a structured abstraction tool developed for this synthesis. The abstraction tool captured the project title, implementation period, geographic setting, population or target group, study or activity type, data source, design where applicable, principal output, current output status, response function, key findings, and operational relevance. For analytic epidemiologic studies, the abstraction captured the study design and main outcome or exposure domains as reported in the project output, but the review did not re-run statistical analyses or pool participant-level data across studies. For outbreak investigation and programmatic activities, the abstraction captured the investigation setting, response questions addressed, output produced, and response-relevant recommendations documented by the project team.
Classification framework
Projects were classified using mpox response functions adapted from national outbreak coordination structures and aligned with World Health Organization functional domains for public health emergency preparedness and response[11]. The response functions were surveillance and case detection, epidemiologic investigations and transmission dynamics, laboratory-epidemiology interface, clinical severity, outcomes, and care models, risk communication and community engagement, health system and workforce capacity, and psychosocial impact and stigma. Classification was based on the public health function addressed by each project rather than on study design alone. Because several projects addressed more than one response function, category assignment was not mutually exclusive; therefore, category totals and percentages could exceed the number of unique projects.
Data synthesis and logic model
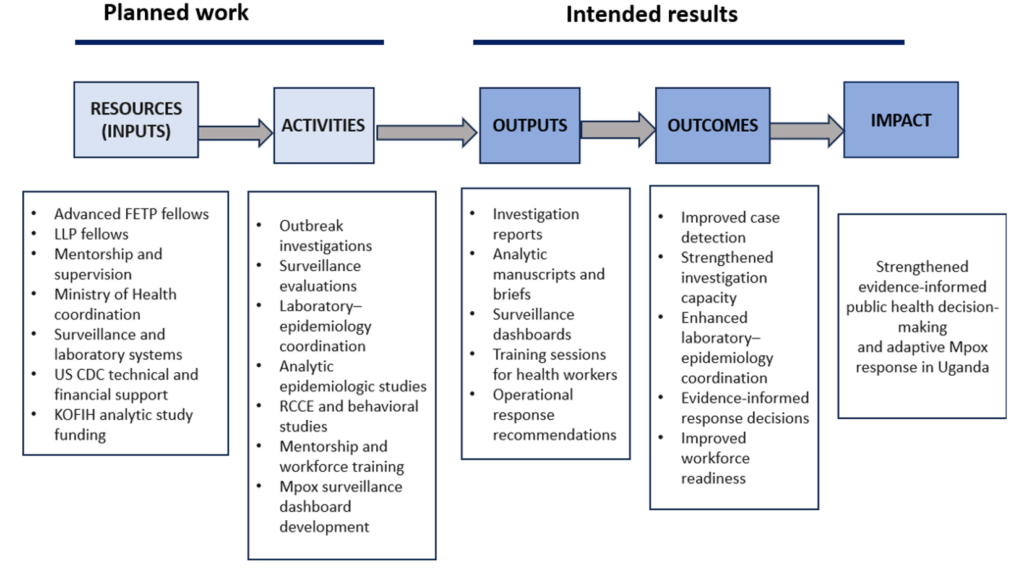
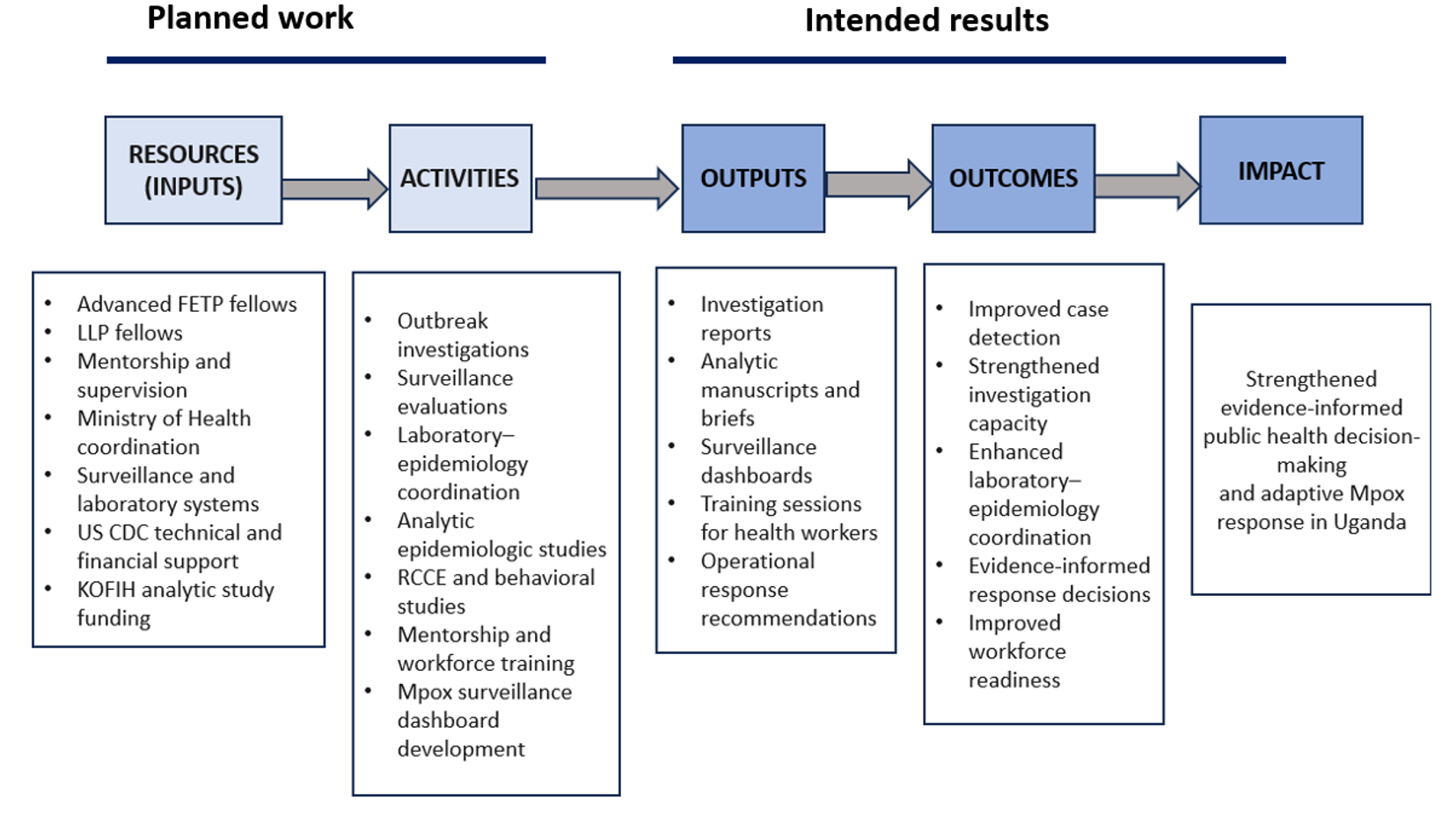
Findings were synthesized thematically across response pillars, with emphasis on operational relevance and contribution to public health decision-making. Where similar findings emerged across multiple projects, results were integrated to avoid duplication and overrepresentation of individual studies. Synthesis focused on identifying recurrent gaps, emerging patterns, and actionable insights that informed response strategies during the outbreak. To guide data synthesis and interpretation, we developed a logic model (Figure 1), informed by recently described impact-evaluation frameworks for Field Epidemiology Training Programs and related public health workforce initiatives [9]. Inputs include the Advanced FETP and LLP workforce, mentorship and technical supervision, institutional support from the Uganda Ministry of Health, and logistical and financial support provided through the United States Centers for Disease Control and Prevention (US CDC) and the Korea Foundation for International Healthcare (KOFIH). Activities include outbreak investigations, surveillance system evaluations, laboratory–epidemiology coordination, analytic epidemiologic studies, mentorship, and risk communication support. Outputs include investigation reports, analytic studies, surveillance dashboards, training activities, and response briefs. Outputs included investigation reports, analytic study reports and manuscripts, surveillance dashboards, training activities, response briefs, and operational recommendations. Outcomes and impact were interpreted as contribution pathways rather than causal effects.
Ethical considerations
All activities included in this synthesis were implemented as part of routine public health surveillance, outbreak investigation, mentorship, program evaluation, or response support under the mandate of the Uganda Ministry of Health. The included activities were reviewed by the US CDC and determined to be non-research public health activities. They were conducted consistent with applicable federal law and CDC policy, including 45 C.F.R. part 46, 21 C.F.R. part 56, 42 U.S.C. section 241(d), 5 U.S.C. section 552a, and 44 U.S.C. section 3501 et seq. No new participant-level data were collected for this synthesis, and no individual-level identifiers are reported in this manuscript.
Overview of included projects
A total of 36 mpox-related response projects met the inclusion criteria. Projects were conducted across multiple epidemiologic and operational settings, including urban and peri-urban areas, island and fishing communities, prisons, health-care facilities, household contexts, and other affected districts (Table 1). The outputs included outbreak investigation reports, surveillance and alert-management evaluations, analytic epidemiologic study reports, laboratory rapid-response assessment outputs, public health bulletin articles, manuscripts, mentorship reports, response briefs, and an operational surveillance dashboard.
Mentorship and capacity-building activities reached approximately 160 health workers across about 30 districts.
Geographic distribution and response functions
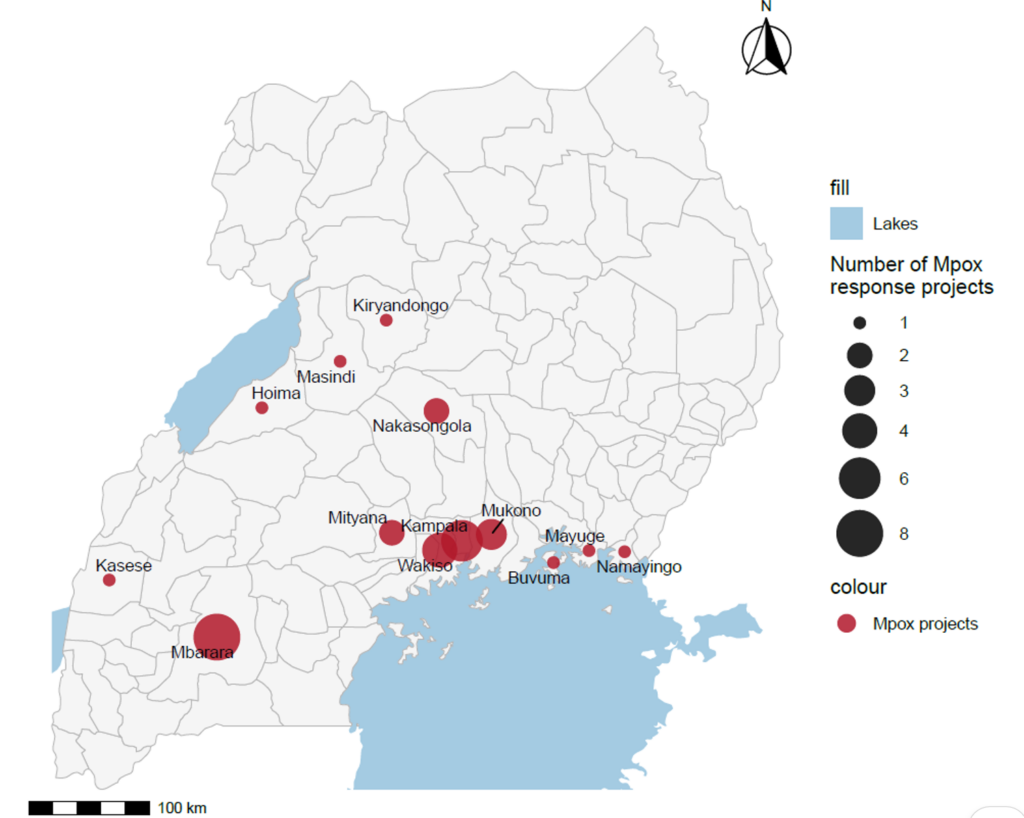
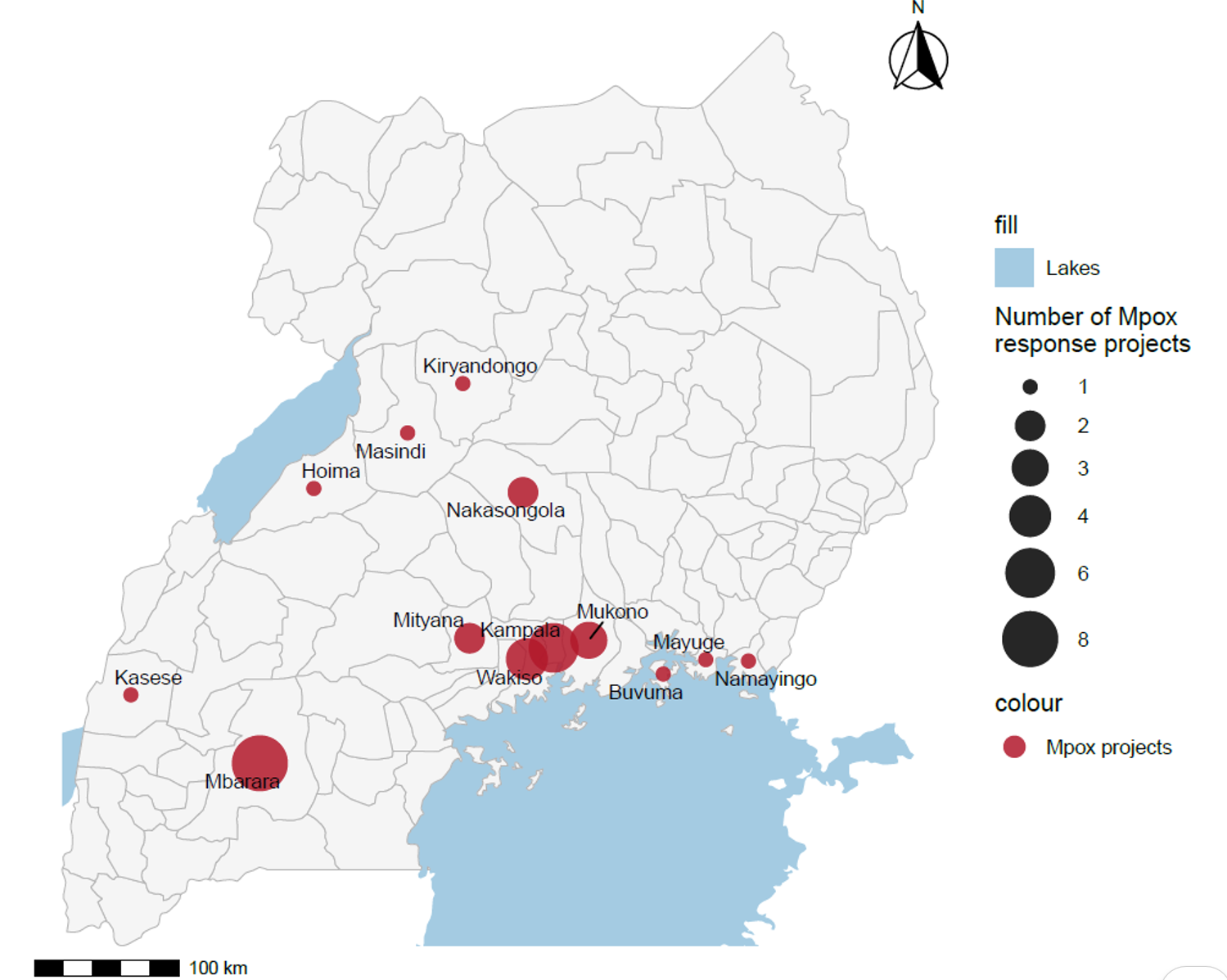
The geographic distribution of projects showed concentration in high-burden response areas, including Mbarara City and the Kampala Metropolitan Area, with additional projects conducted in districts such as Kasese, Mityana, Namayingo, Nakasongola, Buvuma, Mukono, Masindi, Kiryandongo, Hoima, and Mayuge (Figure 2). Among the 36 mpox response projects undertaken, most focused on epidemiologic investigations and transmission dynamics (50%). Other projects addressed clinical severity, outcomes, and care models (33%), surveillance and case detection (19%), laboratory–epidemiology interface activities (11%), risk communication and community engagement (14%), psychosocial impact and stigma (11%), and health system and workforce capacity (8%) (Figure 3).
Mpox response activities and operational contributions of UPHFP fellows
Fellows undertook a broad range of mpox-related response activities between July 2024 and June 2025. These activities generated operationally relevant evidence across surveillance, outbreak investigation, clinical and epidemiologic analysis, community engagement, health system capacity, laboratory–epidemiology coordination, and psychosocial domains. The key operational contributions of these projects to the national mpox response are listed in Table 2.
Surveillance, case detection, and laboratory-epidemiology coordination
Fellows supported surveillance and case-detection activities through alert-management evaluations, documentation reviews, surveillance data-quality assessments, active case-search support, and a national assessment of contact tracing performance. These activities documented gaps in detection, reporting, documentation, and follow-up processes. LLP and Advanced FETP fellows also contributed to laboratory-epidemiology coordination through laboratory rapid-response assessment activities in Greater Mbarara, review of diagnostic and specimen-flow processes, and support for integration of laboratory and epidemiologic information within response outputs. Fellows contributed to the development of a real-time mpox surveillance dashboard that linked epidemiologic and laboratory information for routine monitoring of reported cases by district and region (Table 2).
Epidemiologic investigations and transmission dynamics
Fellows led or supported outbreak investigations and transmission-focused analyses across multiple settings. These included investigations in early outbreak areas, urban and peri-urban transmission settings, island and fishing communities, prison settings, and household contexts. Investigation outputs documented geographic spread, affected populations, transmission contexts, and setting-specific response issues. The findings from these investigations were summarised in project reports, bulletin articles, and manuscripts and are reflected in the response function (Table 2).
Clinical severity, outcomes, and care models
Several projects examined clinical severity, mortality, recovery, delayed isolation, delayed care-seeking, and care models. These included studies of children and adolescents, severity scoring, mortality, time to recovery among hospitalized patients, misdiagnosis, and delayed care-seeking among cases. Other projects examined home-based and facility-based care models and documented implementation issues relevant to infection prevention and follow-up.
Community, behavioural, and risk communication studies
Fellows conducted community and behavioural studies among health-care workers, community health workers, pilgrims, affected communities, and other groups relevant to the response. These activities assessed knowledge, attitudes, practices, vaccine acceptance, infection-prevention practices, reporting behaviours, isolation practices, and barriers to care-seeking. The studies documented response-relevant behavioural and communication issues and provided descriptive insights to tailor risk communication and community engagement activities (Table 2).
Health system and workforce capacity
Fellows contributed to health system and workforce-related activities through mentorship, training, and operational assessments. Mentorship activities focused on mpox surveillance, outbreak investigation, data analysis, and response coordination. Health system assessments documented availability and operational constraints related to personal protective equipment, laboratory turnaround time, isolation capacity, and contact tracing implementation. These findings were summarized in mentorship reports, assessment reports, and the operational contribution synthesis (Table 2).
Several projects documented psychosocial and stigma-related outcomes among mpox survivors and health-care workers. These included studies of anxiety, depression, post-traumatic stress symptoms, stigma, resilience, and perceived occupational risk. The outputs from these projects described mental health and wellbeing issues among affected populations and frontline staff during the response and were included in the psychosocial response-function synthesis (Table 2).
This programmatic review demonstrates that UPHFP fellows contributed across all major functional domains of the mpox response, generating outputs that extended beyond outbreak description to inform surveillance optimisation, laboratory–epidemiology coordination, response targeting, clinical management strategies, community engagement, and health system preparedness. Fellows’ work included supporting diagnostic response through rapid laboratory capacity assessments, improving integration of laboratory and surveillance data, and supporting real-time monitoring of transmission through dashboards linking epidemiologic and laboratory information. These contributions spanned the full course of the mpox outbreak in Uganda, from early detection and characterisation of initial outbreaks through outbreak expansion and into sustained response activities as transmission became established in various settings.
During the early phase of the mpox epidemic, fellows contributed to surveillance, case detection, and laboratory–epidemiology coordination through alert-management evaluations, rapid laboratory response assessments, surveillance data reviews, and analyses of misdiagnosis and under-reporting. These outputs documented operational gaps in diagnostic confirmation, reporting, and coordination between laboratory and surveillance teams, including across public and private healthcare settings [4, 12]. In a newly emerging outbreak with evolving clinical presentation, such outputs were relevant to case verification, isolation planning, and prioritisation of surveillance improvements. They also complemented broader response needs by linking epidemiologic and laboratory information through dashboards and other routine response products.
As transmission expanded geographically, fellows led or supported investigations in urban, peri-urban, fishing, island, institutional, and refugee-hosting settings[12-14]. These investigations described affected populations, transmission patterns, and operational challenges across heterogeneous settings and provided response teams with information relevant to geographic prioritisation, risk communication, and engagement of populations with increased exposure or mobility. This portfolio of outbreak investigations is consistent with the core service role of field epidemiology training programs, which emphasise mentored field practice, descriptive epidemiology, hypothesis generation, and rapid communication of findings during public health emergencies[7, 9].
Published studies and programmatic reports summarised in this review also described clinical severity, mortality, recovery, and care-seeking patterns among mpox patients, including children, adolescents, and persons with comorbidities [3, 15]. These outputs were relevant to discussions on clinical risk stratification, follow-up, and care models during sustained transmission. Evaluations and project reports on home-based and facility-based care documented recovery outcomes and implementation challenges, providing descriptive information for response teams considering context-specific care approaches.
Community and behavioural studies conducted during the response documented knowledge, attitudes, practices, stigma, vaccine concerns, and barriers to isolation and care-seeking among healthcare workers, community health workers, pilgrims, survivors, and affected communities [16-19]. These outputs identified considerations for risk communication and community engagement, particularly as transmission extended beyond early high-risk networks into households and broader community settings. The inclusion of these studies highlights the importance of behavioural and social evidence during outbreaks, especially where delays in care-seeking, stigma, economic constraints, and low perceived risk may influence uptake ofoutbreak response measures.
Mentorship, training, and health system assessments documented the role of UPHFP fellows in response support and workforce development. These activities included mentorship of approximately 160 health workers across 30 districts and assessments describing constraints related to laboratory turnaround time, infection prevention supplies, isolation infrastructure, and contact tracing implementation. These findings are consistent with previous descriptions of Uganda’s fellowship model and its role in supporting outbreak response capacity through embedded service delivery and mentored field practice [8, 10]. Fellows’ mentorship and workforce-strengthening activities during the mpox response align with previous assessments showing that FETPs can simultaneously strengthen workforce capacity while identifying structural health system constraints that require sustained investment [8, 10]. However, because this review did not assess pre- and post-intervention changes, these activities should be interpreted as workforce and response-support contributions rather than measured improvements in system performance.
Importantly, fellows’ work also extended to psychosocial and stigma-related dimensions of the mpox response. Studies documenting mental health outcomes, stigma, and resilience among survivors and healthcare workers expanded the scope of response evidence beyond traditional epidemiologic domains and underscored the importance of integrating psychosocial support into outbreak response planning [20]. The explicit focus on psychosocial outcomes and survivor experiences during the mpox response represents an expansion of documented FETP contributions, reflecting growing recognition of the importance of mental health and workforce resilience during prolonged public health emergencies [21, 22].
The pattern of contributions observed during Uganda’s mpox response is broadly consistent with published evidence on FETP deployments during public health emergencies. Multi-country and programmatic reviews have described FETP contributions to surveillance, outbreak investigation, data analysis, risk communication, and surge support during COVID-19 [7, 10, 23, 24] and other emergencies [25-30].Similar contributions have been described during Uganda’s COVID-19 response, where trainees supported surveillance systems, dashboards, contact tracing evaluation, behavioural studies, and workforce training [31-35]. The Uganda mpox response adds to this literature by documenting a combined field epidemiology and laboratory leadership contribution through UPHFP, including laboratory–epidemiology coordination, survivor-focused studies, and psychosocial assessments.
Uganda’s mpox response also reflected institutional learning from previous large-scale outbreaks, particularly COVID-19 and Ebola. Prior outbreak responses in Uganda documented the value of transmission analyses, household investigations, institutional outbreak investigations, behavioural studies, and health worker wellbeing assessments [10, 36-38]. The mpox response drew on similar approaches, including studies on household transmission, care-seeking, stigma, survivor mental health, and healthcare worker resilience. These parallels suggest that embedding analytic and programmatic studies within outbreak responses can help preserve institutional memory and support preparedness.
The findings from this review have broader implications for how countries design and sustain epidemic preparedness systems. The findings support the value of field epidemiology and laboratory leadership training programs as response-support platforms that can provide analytic, operational, and workforce contributions during public health emergencies. Embedding trainees within national and subnational response systems creates a mechanism through which routine training, mentored service delivery, and emergency response can reinforce each other. For Uganda and similar settings, sustained investment in advanced field epidemiology, laboratory leadership, and related public health workforce programs could improve readiness for future epidemics by ensuring that skilled personnel are available to support surveillance, field investigation, laboratory coordination, data use, and response adaptation when similar large-scale outbreaks occur. Future evaluations should move beyond documenting outputs to assess how these workforce models influence response timeliness, quality, coordination, and public health outcomes.
Limitations
This review has several limitations. First, the projects synthesised were heterogeneous in scope, design, methods, scale, and documentation quality, reflecting the realities of conducting operational work during an active public health emergency. As a result, findings across projects were not directly comparable, and this review should be interpreted as a descriptive synthesis of response activities rather than a pooled analysis of study outcomes.
Second, because this was a descriptive programmatic review, we did not assess the independent effect of fellows’ activities on outbreak outcomes such as time to detection, transmission, morbidity, mortality, response efficiency, or health system performance. The findings therefore represent contributions to response functions, not causal attribution of response improvements to UPHFP fellows alone.
Third, mpox response activities were implemented collaboratively by the Uganda Ministry of Health, Uganda National Institute of Public Health, district health teams, laboratories, implementing partners, and multiple response pillars. This collaborative response structure limits attribution of specific outputs or decisions solely to Advanced FETP or LLP fellows.
Fourth, this synthesis focused on activities undertaken by Advanced FETP and LLP fellows and did not capture contributions from other UPHFP tracks, frontline and intermediate field epidemiology training tiers, district surveillance teams, laboratory networks outside LLP, or the broader public health workforce. The findings therefore describe only a defined subset of workforce contributions during the mpox response.
Finally, documentation completeness varied across projects. Some activities prioritised rapid operational reporting, field response, mentorship, or dashboard development over detailed manuscript-style documentation, and some output remained unpublished or under review at the time of synthesis. To reduce overinterpretation, unpublished outputs were treated as programmatic response documents rather than peer-reviewed evidence.
UPHFP fellows were an important component of Uganda’s mpox response workforce during 2024–2025, contributing across surveillance, outbreak investigation, laboratory–epidemiology coordination, clinical analysis, risk communication, workforce mentorship, and psychosocial domains. Their embedded role within response structures provided operational and analytic support across multiple phases of the epidemic. These findings support continued investment in field epidemiology and laboratory leadership training programs as part of national epidemic preparedness and response capacity.
What is already known about the topic
Field Epidemiology Training Programs (FETPs) provide surge workforce capacity for outbreak detection, investigation, and response.
Evidence describing the collective contributions of FETP trainees across multiple response pillars during large-scale outbreaks remains limited, particularly in Africa.
What this study adds
During Uganda’s 2024–2025 Mpox outbreak, Advanced FETP and Laboratory Leadership Program fellows completed several projects spanning surveillance, outbreak investigation, laboratory coordination, clinical outcomes, risk communication, and health systems strengthening.
Findings informed public health decision-making, identified surveillance and diagnostic gaps, and guided targeted response interventions.
The study highlights a practical model for leveraging FETPs as workforce surge capacity to strengthen preparedness and response to emerging and re-emerging infectious disease threats in resource-limited settings.
Lilian Bulage is an Associate Editor at the Journal of Interventional Epidemiology and Public Health (JIEPH) and a co-author of this manuscript. In line with the journal’s conflict of interest policy, she was fully recused from the peer review process and had no involvement in editorial handling or decision-making for this submission. An independent editor oversaw the review and decision-making process. The other authors declare that they have no competing interests.
Availability of data and materials
The datasets generated and analysed during the current study are derived from routine outbreak investigation reports, surveillance summaries, and programmatic outputs produced as part of the national mpox response and are available from the corresponding author upon reasonable request and with permission from the Uganda Ministry of Health.
Uganda’s Advanced Field Epidemiology Training Program and Laboratory Leadership Program are implemented by the Uganda Ministry of Health through the Uganda National Institute of Public Health with technical and financial support from the United States Centres for Disease Control and Prevention. Additional support for mpox-related analytic studies conducted during the outbreak response was provided by the Korea Foundation for International Healthcare. The funders had no role in the design of this review, data synthesis, interpretation of findings, or writing of the manuscript.
We acknowledge the Uganda Ministry of Health for its leadership of the Mpox response and the UPHFP fellows for their contributions to outbreak investigation and response activities. We also acknowledge district health teams, surveillance officers, laboratory personnel, and implementing partners who supported Mpox response activities across Uganda.
| No | Period | Activity / project title | Project type or data source | Response function(s) | Output used for synthesis |
|---|---|---|---|---|---|
| 1 | July-August 2024 | Investigation of the first confirmed Mpox outbreak in Kasese District, western Uganda | Outbreak investigation report; descriptive field investigation | Epidemiologic investigation; surveillance and case detection | Completed outbreak investigation report; manuscript under review |
| 2 | July-October 2024 | Factors associated with Mpox severity in Uganda (MPSSS validation) | Analytic epidemiologic study using national Mpox case data | Clinical severity, outcomes, and care models | Completed analytic study; manuscript in preparation; public health bulletin article[15] |
| 3 | July-December 2024 | Delayed patient isolation and associated factors during the Mpox outbreak in Uganda | Analytic epidemiologic study using case investigation and isolation data | Surveillance and case detection; RCCE | Completed analytic study report; manuscript published [4] |
| 4 | July 2024-February 2025 | Evaluation of performance and impact of contact tracing during the Mpox outbreak in Uganda | National program evaluation using contact tracing records | Surveillance and case detection; health system and workforce capacity | Completed national evaluation report; manuscript in preparation |
| 5 | July 2024-February 2025 | Risk factors for Mpox transmission among household contacts in Uganda | Analytic epidemiologic study among household contacts | Epidemiologic investigation and transmission dynamics | Completed analytic study; manuscript in preparation |
| 6 | August-September 2024 | Epidemiological profile of early Mpox cases in Uganda | Descriptive analysis of early national case data | Surveillance and case detection; epidemiologic investigation | Completed descriptive epidemiologic analysis; manuscript under review |
| 7 | August-September 2024 | Assessment of healthcare workers knowledge, attitudes, and practices toward Mpox in Uganda | Cross-sectional KAP study among healthcare workers | Risk communication and community engagement; workforce readiness | Completed analytic report; manuscript under review; public health bulletin article [16] |
| 8 | August-October 2024 | Psychological distress and perceived Mpox risk among healthcare workers during early outbreak phase | Cross-sectional psychosocial assessment among healthcare workers | Psychosocial impact and stigma; healthcare worker wellbeing | Completed analytic report; manuscript under review |
| 9 | August-September 2024 | Mpox outbreak investigation in fishing communities of Nakasongola District | Outbreak investigation report; descriptive field investigation | Epidemiologic investigation and transmission dynamics | Completed outbreak investigation report; manuscript in preparation; public health bulletin article [12] |
| 10 | August 2024-January 2025 | Epidemiology, clinical features, and outcomes of Mpox in children and adolescents in Uganda | Analytic study of pediatric and adolescent case data | Clinical severity, outcomes, and care models | Completed analytic study; manuscript published [3] |
| 11 | August 2024-January 2025 | Stigma and associated factors among Mpox survivors in Kampala Metropolitan Area | Cross-sectional study among Mpox survivors | Psychosocial impact and stigma | Completed analytic study; public health bulletin article; manuscript published [19] |
| 12 | August 2024-May 2025 | Factors associated with Mpox-related mortality in Uganda | Analytic epidemiologic study using national case outcome data | Clinical severity, outcomes, and care models | Completed analytic study; manuscript in preparation |
| 13 | September-October 2024 | Coordinated outbreak investigations in Mityana and Namayingo Districts | Coordinated district outbreak investigation reports | Epidemiologic investigation and transmission dynamics | Completed investigation reports; programmatic outputs |
| 14 | September-October 2024 | Investigation of Mpox outbreak in Mityana District, Uganda | District outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 15 | September-October 2024 | Mpox outbreak investigation in Namayingo District | District outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 16 | October 2024 | Mpox outbreak investigation in prison settings (Masindi Prison) | Institutional outbreak investigation report | Epidemiologic investigation and transmission dynamics; health system capacity | Completed outbreak investigation report; public health bulletin article [13] |
| 17 | October 2024-January 2025 | Evaluation of alert management system during Mpox response in Kampala Metropolitan Area | Surveillance system evaluation using alert management records | Surveillance and case detection | Completed evaluation report; manuscript in preparation |
| 18 | October 2024-March 2025 | Mpox outbreak investigation in Mbarara City, Uganda | City outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed outbreak investigation report; public health bulletin article [39] |
| 19 | October 2024-May 2025 | Mpox outbreak investigation in Greater Mbarara (urban and peri-urban settings) | Analytic synthesis of outbreak investigation data | Epidemiologic investigation and transmission dynamics | Completed analytic synthesis; manuscript under review[20] |
| 20 | October 2024-May 2025 | Laboratory rapid response assessment and intervention during the Mpox outbreak in Greater Mbarara, Uganda | Laboratory rapid response assessment and intervention documentation | Laboratory-epidemiology interface | Laboratory assessment and intervention report; programmatic output |
| 21 | October 2024-May 2025 | Factors associated with Mpox misdiagnosis in Mbarara City | Analytic epidemiologic study using clinical encounter data | Laboratory-epidemiology interface; surveillance and case detection | Completed analytic study; public health bulletin article[40] |
| 22 | October 2024-April 2025 | Predictors of time to recovery among Mpox patients admitted at Mbarara Regional Referral Hospital | Analytic study among hospitalized Mpox patients | Clinical severity, outcomes, and care models | Completed analytic study; manuscript in preparation |
| 23 | October-November 2024 | Mpox case investigations in Kampala Metropolitan Area (Mukono, Wakiso, Kampala) | Case investigation reports across Kampala Metropolitan Area | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 24 | November 2024 | Mpox outbreak investigation at Sowe Island, Mukono District | Island outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed outbreak investigation report; public health bulletin article [14] |
| 25 | December 2024 | Individual and household factors of Mpox among household contacts in Nakasongola and Mayuge Districts | Analytic report among household contacts | Epidemiologic investigation and transmission dynamics; RCCE | Completed analytic report; programmatic output |
| 26 | January-February 2025 | Resilience and associated factors among healthcare workers in Mpox treatment units | Cross-sectional assessment among healthcare workers | Psychosocial impact and stigma; workforce wellbeing | Completed analytic study; manuscript under peer review |
| 27 | January-February 2025 | Post-traumatic stress disorder, depression, and anxiety among Mpox survivors in central Uganda | Cross-sectional psychosocial assessment among survivors | Psychosocial impact and stigma | Completed analytic study; manuscript in preparation |
| 28 | February 2025 | Knowledge, attitudes, and practices of community health workers regarding Mpox in Mbarara City | Cross-sectional KAP study among community health workers | Risk communication and community engagement | Completed analytic study; manuscript published [41] |
| 29 | February 2025 | Prevalence and determinants of Mpox vaccine acceptance among healthcare workers in Kampala Metropolitan Area | Cross-sectional study among healthcare workers | Risk communication and community engagement | Completed analytic study report; public health bulletin article [18] |
| 30 | February-March 2025 | Enhancing capacity for Mpox surveillance through mentorship in high-risk districts | Mentorship and training reports | Health system and workforce capacity; surveillance and case detection | Mentorship reports; training of approximately 160 health workers |
| 31 | March 2025 | Epidemiological investigation of Mpox outbreak on Lyabana Island, Buvuma District | Island outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 32 | April 2025 | Mpox outbreak investigation in Kiryandongo District and Hoima City | District and city outbreak investigation report | Epidemiologic investigation and transmission dynamics | Completed investigation report; programmatic output |
| 33 | May 2025 | Factors associated with delayed care-seeking among Mpox cases in Mbarara City | Analytic epidemiologic study using case investigation data | Clinical severity, outcomes, and care models; RCCE | Completed analytic study; manuscript under development |
| 34 | May 2025 | Prevalence and factors associated with Mpox severity in Nyamityobora ward, Mbarara City | Analytic study using ward-level case data | Clinical severity, outcomes, and care models | Completed analytic study; manuscript in preparation |
| 35 | June 2025 | Knowledge, attitudes, and practices on Mpox among pilgrims during Martyrs Day commemoration | Cross-sectional KAP assessment among pilgrims | Risk communication and community engagement | Completed analytic report; manuscript in preparation |
| 36 | 2024-2025 | Development of a real-time Mpox surveillance dashboard in collaboration with the United States CDC | Operational dashboard development and surveillance data integration | Surveillance and case detection; laboratory-epidemiology interface | Operational dashboard implemented |
Note. Response functions are not mutually exclusive; a project could contribute to more than one response function where applicable. Output status refers to outputs available for this synthesis at the time of manuscript preparation; unpublished reports are programmatic response outputs, not peer-reviewed publications.
| Response function / operational focus | Project outputs contributing to this domain | Descriptive findings from project outputs | Response relevance or recommendations from project outputs |
|---|---|---|---|
| Under-reporting and misdiagnosis | Misdiagnosis study in Mbarara City; delayed isolation analysis; surveillance reviews | Project outputs documented delayed recognition and frequent initial alternative diagnoses, especially in private facilities. | Supported recommendations for targeted orientation of private facilities, dissemination of case definitions, and Mpox screening in outpatient settings. |
| Alert management and surveillance performance | Kampala Metropolitan Area alert-management evaluation; surveillance data quality reviews | Project outputs documented alert triage, documentation, and timeliness gaps. | Supported recommendations for improving alert documentation, triage procedures, and routine data quality review. |
| Laboratory-epidemiology coordination and diagnostic response | Greater Mbarara laboratory rapid response assessment; dashboard development; diagnostic-delay related studies | Project outputs documented sample transport, turnaround time, and coordination constraints between surveillance and laboratory teams. | Supported recommendations to improve specimen referral, laboratory turnaround time monitoring, and integration of laboratory and epidemiologic data. |
| Early transmission dynamics | District outbreak investigations in Kasese, Nakasongola, Mbarara, KMA, Mukono, Masindi Prison, Mityana, Namayingo, Buvuma, Hoima, and Kiryandongo | Project outputs described transmission patterns across urban, fishing, island, institutional, and community settings. | Supported geographic prioritization of response activities and population-specific risk communication. |
| Household and non-sexual transmission | Household-contact analyses; home-based-care related assessments | Project outputs documented transmission in household settings and potential exposure through close contact and shared items. | Supported recommendations to extend messaging beyond sexual networks to households, caregivers, and home-based care settings. |
| Pediatric Mpox | Analysis of children and adolescents with Mpox | Project outputs described clinical features and outcomes among children and adolescents. | Supported recommendations for pediatric-focused clinical guidance and school/community messaging. |
| Delayed care-seeking and isolation | Delayed isolation analysis; delayed care-seeking analysis in Mbarara City | Project outputs documented delayed care-seeking, delayed isolation, and barriers including self-medication, low perceived risk, and access constraints. | Supported recommendations for early-care-seeking messages and frontline diagnostic orientation. |
| Clinical severity, mortality, recovery, and care models | Severity analysis; mortality analysis; recovery-time analysis; home-based and facility-based care evaluations | Project outputs described patterns of severity, mortality, recovery, and care model implementation. | Supported recommendations for risk stratification, referral prioritization, and context-specific case management planning. |
| Contact tracing implementation | National contact tracing evaluation | Project outputs documented initiation, follow-up, completion, and implementation constraints in contact tracing. | Supported recommendations to refine contact tracing procedures and align resources with feasible response strategies. |
| Health system and workforce capacity | Mentorship and training reports; health system assessments; PPE, isolation, and operational support reviews | Project outputs documented workforce training coverage and operational constraints affecting response activities. | Supported recommendations for emergency logistics, training, supervision, and workforce support. |
| Risk communication and community engagement | KAP studies among health workers, community health workers, pilgrims, and affected communities; vaccine acceptance study | Project outputs documented gaps in knowledge, reporting, referral, prevention practices, and vaccine concerns. | Supported recommendations for targeted RCCE messages for health workers, community health workers, mobile populations, caregivers, and communities. |
| Psychosocial impact, stigma, and survivor wellbeing | Stigma study among survivors; PTSD, depression, and anxiety study; healthcare worker psychosocial assessments | Project outputs documented stigma, mental health symptoms, and psychosocial concerns among survivors and healthcare workers. | Supported recommendations to integrate psychosocial support and stigma reduction into Mpox care and response pathways. |
| Healthcare worker resilience and occupational wellbeing | Resilience study among healthcare workers in Mpox treatment units; psychological distress assessment | Project outputs documented occupational stressors, perceived risk, and resilience-related concerns among frontline workers. | Supported recommendations for infection prevention support, staff wellbeing interventions, and resilience-oriented supervision. |
RCCE, risk communication and community engagement; PPE, personal protective equipment; KMA, Kampala Metropolitan Area; PTSD, post-traumatic stress disorder.